
The 'Telehealth-Ready' Collaborator: Managing Multi-State Compliance
📌 Key Takeaways
Multi-state telehealth compliance hinges on patient location, not provider location—each state where patients are physically present during visits imposes its own licensure and collaboration requirements.
Patient Location Determines Jurisdiction: Legal compliance is governed by where the patient sits during the telehealth visit, requiring state-specific NP licensure and appropriately licensed collaborating physicians for each jurisdiction.
Documentation Trumps Signatures: State boards audit for evidence of active collaboration—documented chart reviews, secure communication trails, and organized records—not just signed agreements sitting in filing cabinets.
Network Models Enable Scalability: Multi-state expansion requires either building fragile individual physician relationships in each state or partnering with networks that maintain pre-established coverage across target jurisdictions.
Controlled Substances Require Verification: Federal telemedicine prescribing regulations expire and renew periodically, with the Third Temporary Rule ending December 31, 2024, making 2026 status verification essential before prescribing across state lines.
CPA Portfolio Management Prevents Chaos: Treating collaborative practice agreements as a tracked portfolio—with renewal dates, chart review cadences, and backup coverage plans documented—transforms compliance from memory exercise into systematic process.
Collaboration is infrastructure, not just a signature.
Independent nurse practitioners and physician assistants expanding telehealth services across state lines will gain actionable compliance frameworks here, preparing them for the detailed implementation runbook that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
You added telehealth to expand access. Now you're wondering if you accidentally expanded your compliance risk instead.
It's a familiar moment. You launched virtual care to reach more patients. The technology works. The appointments fill. Then someone books from Ohio—and your NP license covers Pennsylvania. Your collaborating physician? Also Pennsylvania-based. The question hits hard: Is this legal?
A telehealth-ready collaborating physician partnership reduces multi-state compliance risk by ensuring state-matched licensure and audit-ready oversight workflows for every patient location. Instead of scrambling to rebuild your practice infrastructure each time you add a state, you build once using a systematic approach that scales.
Here's the practical runbook you can use each time you add a state—without rebuilding your practice from scratch.
What a "Telehealth-Ready" Collaborator Actually Is (and What It Isn't)
A telehealth-ready collaborator is a physician partner (or network) who is licensed where your patient is located, can support state-specific oversight requirements, and has an operational process that holds up under scrutiny.
It's not a "national" supervising relationship. There's no universal collaboration credential that travels across state lines. Think of it this way: telehealth makes your office everywhere—but licenses don't travel. Each state where you treat patients applies its own rules for NP practice authority, collaborating physicians, and prescriptive privileges.
Here's what this looks like in practice:
Good: One state, one Collaborative Practice Agreement (CPA), basic chart review process
Better: Two states, two state-specific CPAs, scheduled review cadence with documented communication
Best: Multi-state network coverage with a standardized "audit binder" approach that demonstrates active oversight in every jurisdiction
The difference between "good" and "best" isn't just paperwork. It's the infrastructure that protects your license when a state board asks to review your telehealth arrangements.
The Core Rule: Your Patient's Location Drives Your Compliance Obligations
Telehealth care delivery is regulated by the laws of the state where the patient is located at the time of care. This isn't intuitive—most providers assume their own office location sets the rules—but it's the foundational principle that drives everything else. The Department of Health and Human Services explicitly emphasizes that legal jurisdiction is determined by the patient's physical location at the time of service, dictating which state rules apply.
Build your compliance plan around patient location, not your office location. When a patient in New Jersey connects to your virtual visit, you're practicing under New Jersey's laws for that encounter. This affects three critical areas: your NP licensure requirements, collaboration or supervision arrangements, and prescribing authority (especially for controlled substances).
Multi-state NP telehealth practice requires state-specific licensure and, when required by that state's scope of practice laws, state-valid collaboration arrangements. A Pennsylvania-licensed collaborating physician cannot provide the legally required oversight for your New Jersey patients if New Jersey requires collaboration and specifies that the collaborating physician must hold an active New Jersey medical license.
Do this now: List every state where you plan to see patients. This is your compliance footprint—and it defines the scope of your oversight needs.
Step-by-Step: A Practical Multi-State Compliance Runbook
You can operationalize multi-state telehealth compliance with a repeatable runbook each time you add a state. Follow these eight steps:
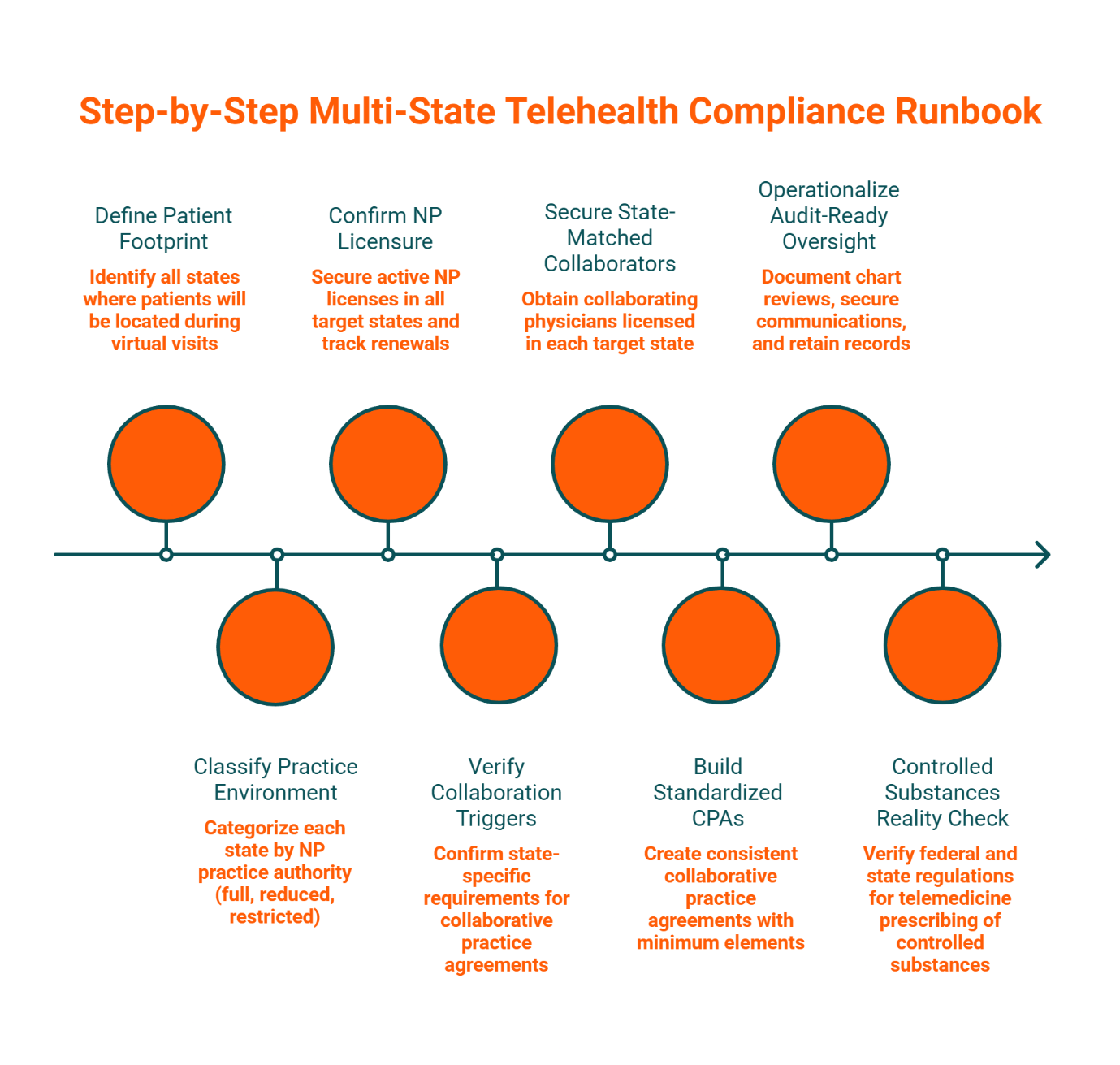
1. Define Your Patient Footprint
Identify all states where patients will be located during virtual visits. Don't guess—check your scheduling software, intake forms, and billing records to confirm where demand actually exists.
2. Classify Each State's NP Practice Environment
States fall into three categories: full practice authority (no physician collaboration required), reduced practice (collaboration required after a transition period), or restricted practice (ongoing collaboration or supervision required). The American Association of Nurse Practitioners maintains the authoritative state-by-state breakdown of these practice environments.
3. Confirm Your NP Licensure and Renewal Cadence
Secure an active NP license in every state where you'll treat patients. Track renewal dates in a central calendar—a lapsed license is an immediate compliance failure that can trigger credentialing issues with payers and platforms.
4. Confirm Collaboration or CPA Triggers
For states with reduced or restricted practice authority, verify whether state law requires a written collaborative practice agreement, specifies chart review frequencies, mandates specific clinical protocols, or requires physician availability for consultation. State medical and nursing boards publish these requirements.
5. Secure State-Matched Collaborating Coverage
When collaboration is required, the collaborating physician's medical license must align with the state where the patient is located. One local physician often cannot cover your entire telehealth footprint. This is where a multi-state network becomes essential—you need access to physicians licensed in each of your target states.
6. Build or Standardize Your CPAs
Every CPA should include these minimum elements: scope of practice, chart review process and percentage of charts reviewed, availability and consultation protocols, termination notice requirements, and documentation retention obligations. Consistency across agreements makes audits manageable.
7. Operationalize "Audit-Ready" Oversight
Clear CPA terms demonstrate active oversight during audits. Document your chart review process with timestamps, maintain secure communications with your collaborating physician (encrypted messaging, scheduled video conferences), and retain all documentation in an organized system. The compliance risk isn't usually lack of knowledge—it's the lack of a consistent operational trail.
8. Controlled Substances Reality Check
Telemedicine prescribing requirements for controlled substances can change at both federal and state levels. Before offering telehealth services that include prescribing across state lines, verify the current regulations and individual state requirements. Federal regulations regarding the telemedicine prescribing of controlled substances are subject to expiration and renewal. While the DEA previously implemented temporary extensions to ensure continuity of care (such as the Third Temporary Rule which extended flexibilities through December 31, 2024), providers must verify the specific federal status effective for 2026. Note that even if federal law permits remote prescribing, individual states may impose stricter in-person requirements.
Managing Multiple CPAs Without Chaos
Multi-state practice becomes manageable when you treat CPAs like a portfolio rather than individual agreements scattered across filing cabinets.
Create a simple CPA portfolio tracker with these columns: the state designation, effective date paired with renewal date, chart review cadence specified as both frequency and percentage of charts sampled, a coverage backup plan detailing what happens if the collaborating physician is unavailable, the termination notice period typically ranging from 30 to 90 days, and the documentation location identifying where your audit binder for this state is stored.
This tracker transforms compliance from a memory exercise into a systematic process. You can see at a glance which agreements need renewal, which states require action this month, and where your coverage gaps exist before they become emergencies.
A scalable collaboration network enables adding new states without rebuilding oversight from scratch. Instead of searching for individual physicians every time you expand, you work with a service that maintains multi-state coverage and handles the operational complexity of coordinating multiple agreements.
Operationalizing Oversight for Telehealth (Chart Review, Secure Communications, HIPAA)
The operational reality matters more than the signed agreement. State boards conducting audits want evidence of active collaboration—not just a signature on file.
Here's what an "audit-ready month" looks like in practice:
You upload charts for review through a HIPAA-compliant system on a documented schedule
You can reach your collaborating physician securely through encrypted text messaging, phone calls, or video conferences when clinical questions arise
You maintain a documented cadence (monthly or quarterly, depending on state requirements and CPA terms) with dated records of all interactions
Physician Collaborators structures this process to meet these operational standards: providers upload charts through a secure, HIPAA-compliant portal, communicate via encrypted channels, and schedule Zoom conferences for more hands-on practice guidance when needed. The services are designed specifically for independent NP and PA telehealth practices that need this level of systematic support.
The goal is simple: if a board auditor requests your collaboration documentation tomorrow, you can provide a complete, organized record within hours—not days of frantic searching.
Choosing the Right Collaboration Model: Single Physician vs. Network
If you're staying in one state with stable patient volume, a single state-aligned collaborating physician may be sufficient. The relationship is direct, the communication is simple, and the overhead is minimal.
If you're adding states or planning to expand your telehealth footprint, you need scalability. Here's the decision framework:
Are you treating patients in more than one state?
No → A single collaborating physician licensed in your practice state can provide the required oversight. Focus on finding a physician whose specialty aligns with your practice area and who understands telehealth workflows.
Yes → You need a multi-state coverage strategy. This typically means either building relationships with individual physicians in each state (time-intensive and fragile if any physician becomes unavailable) or working with a network service that maintains coverage across your target states.
Addressing the "Signature-Only" Risk
Some providers are tempted by the cheapest option: a physician who signs a CPA and provides minimal oversight. Signature-only arrangements increase audit and continuity risk in states with restricted or reduced practice authority. If a state board audits your practice and finds no documented chart review, no communication trail, and no evidence of actual collaboration, the signed agreement provides no protection. The chain of risk flows directly to credentialing disruption, which leads to revenue interruption when payers suspend your participation or telehealth platforms remove your access.
Why an "Employee Medical Director" Often Doesn't Fit
On the opposite end, some advisors recommend hiring a physician as a full-time or part-time employee to serve as your practice's medical director. For large, established practices, this model provides maximum control and integration. For independent NPs running lean telehealth operations, it's often unnecessary overhead—you're paying for infrastructure you don't need. The network or fractional collaboration model functions as your agile, scalable alternative: you get the expertise and coverage without the employment complexity, benefits administration, or fixed salary commitment.
The right model depends on your specific situation, but the principle remains constant: collaboration is infrastructure, not just a signature.
Telehealth Expansion Checklist
Use this checklist each time you add a new patient state to your telehealth practice:
Before Treating Patients in a New State:
[ ] Confirm the state's NP practice authority classification (full / reduced / restricted practice)
[ ] Obtain active NP licensure in the new state
[ ] Verify whether state law requires a collaborative practice agreement or physician oversight
[ ] If collaboration is required, confirm that your collaborating physician holds an active medical license in that state
[ ] Review state-specific prescribing requirements, especially for controlled substances
[ ] Establish or update the CPA to include state-specific protocols if required
[ ] Set up the chart review process and documentation system for the new state
[ ] Update your professional liability insurance to confirm coverage for the new state
[ ] Notify relevant payers and credentialing bodies of your expanded practice location
[ ] Add the state to your CPA portfolio tracker with renewal dates and review requirements
This checklist is designed to stand alone as a quick reference.
FAQ: Common Multi-State Questions NPs Ask
Can my collaborating physician be in a different state than my patient?
Yes—physically, they can be anywhere. However, legally, they must hold a valid medical license in the state where the patient is located.
Do I need a CPA for every state?
It depends on the state's practice authority laws. States with full practice authority for NPs generally don't require collaboration. States with reduced or restricted practice authority do. You need a separate CPA (or an amendment to your existing agreement) for each state that requires collaboration, and the collaborating physician must be licensed in that state.
How often should chart review happen?
State requirements vary, but common standards include monthly or quarterly review of 5-10% of patient charts. Your CPA should specify the exact percentage and frequency. The key is consistency—document every review with dates, findings, and any follow-up actions.
What's the fastest way to add one new state without breaking compliance?
Start with the checklist above. The timeline depends on NP licensure processing times (which can range from a few weeks to several months) and securing a state-matched collaborating physician. Working with a network that already has coverage in your target state can reduce the physician-matching timeline to about one week, but the licensure timeline is controlled by state boards.
Ready to build audit-ready multi-state coverage? Book your free consultation to discuss your specific telehealth footprint and collaboration needs. Physician Collaborators matches you with board-certified physicians licensed in your target states, typically within one week, with pricing in the range of $500-$1,250 per month depending on your practice scope.
Disclaimer: This guide is intended as a comprehensive starting point. For decisions specific to your unique situation, we always recommend consulting a qualified professional.
About the Physician Collaborators Insights Team
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.