
The NJ/NY/PA Protocol: Specific Collaboration Requirements for Tri-State NPs
📌 Key Takeaways
Independent nurse practitioners serving patients across New Jersey, New York, and Pennsylvania need state-specific collaboration documentation for each jurisdiction where they practice.
One Document Per State Rule: Each state requires distinct paperwork—New Jersey protocols for prescribing, New York's Form 4NP or autonomous pathway documentation, and Pennsylvania's written collaborative agreement structure—making universal templates a credentialing liability.
Patient Location Drives Compliance: Telehealth encounters follow the rules of the state where the patient sits, not where the provider practices, requiring separate compliance folders and routing protocols for cross-border care.
Proof Beats Signatures Alone: Audit-ready collaboration means documented chart reviews, consultation logs, and availability records that prove oversight actually occurred, not just theoretical agreement on paper.
Tri-State Physicians Need Tri-State Licenses: A collaborating physician can only cover patients in states where they hold active medical licensure, eliminating shortcuts where one NJ license attempts to cover NY or PA practice.
State-matched documents plus defensible oversight equals credentialing confidence.
Independent NPs and PAs launching or expanding multi-state telehealth practices will find implementation-ready compliance protocols here, preparing them for the state-by-state breakdown that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
Three states. Three patient populations. One unanswered question: do you need three different collaboration setups?
If you're an independent Nurse Practitioner serving patients across New Jersey, New York, and Pennsylvania—whether in-person, via telehealth, or both—the answer is more nuanced than most people realize. State-licensed physician oversight for NPs isn't a one-size-fits-all requirement. It's like having three local guides who each know the specific terrain and laws of their territory. The provision of this oversight must match the specific jurisdiction where you're practicing to meet local practice mandates. Practicing with the certainty that you're fully compliant with your specific state's complex medical board rules means selecting a physician licensed in your specific state of practice and maintaining documentation that proves the oversight relationship exists and functions as required.
Here's what that means in practice: build one compliance folder per state, keep your oversight routine documented, and know which rulebook applies when a patient crosses state lines.
Do You Need Different Collaboration Documents for NJ, NY, and PA?
Yes, in most cases. Each state has its own statutory framework for NP practice and prescribing authority, which means the documents, oversight expectations, and proof-of-compliance requirements differ across state lines.
Consider this scenario: you're an NP running a psychiatric telehealth practice. You see New Jersey patients in your office, serve New York patients remotely, and occasionally treat Pennsylvania residents who live near the border. You'll need NJ-specific documentation for your in-state prescribing, a NY practice agreement structure that satisfies their consultation and review requirements, and a written PA collaborative agreement that meets their regulatory model. One physician might be able to serve all three states if they hold active licenses in each—but the paperwork, protocols, and documentation expectations are distinct for each jurisdiction.
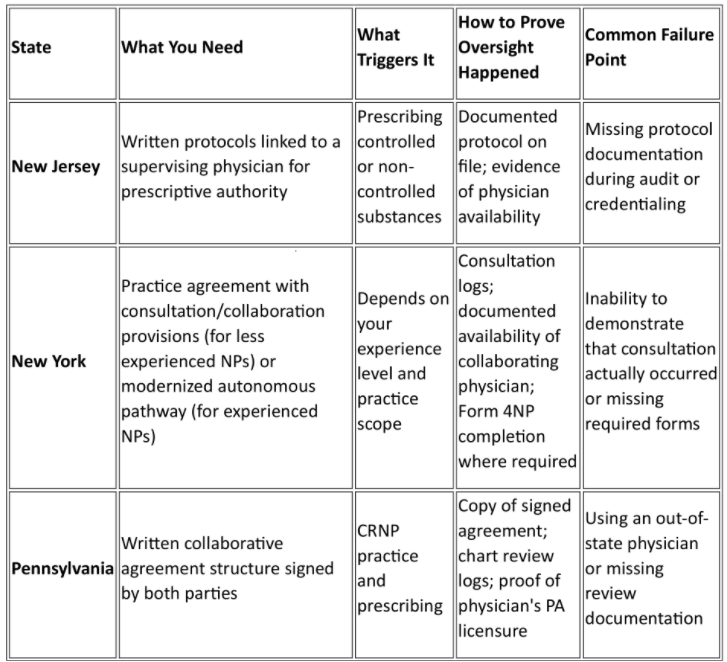
The Tri-State Compliance Cheat Sheet
Requirements by State
Your Keep-on-File Folder (One Per State)
For each state where you see patients, maintain:
Signed agreement or protocol (state-specific format)
Collaborator's license verification (confirm active status in that state)
Chart review logs (dates, sample size, findings)
Availability/coverage expectations (documented communication channels)
Malpractice coverage alignment (confirm your collaborator's policy covers their supervisory role)
Renewal reminders (most agreements expire annually or biennially)
New Jersey: What Triggers a Required Physician Relationship (and What to Keep on File)
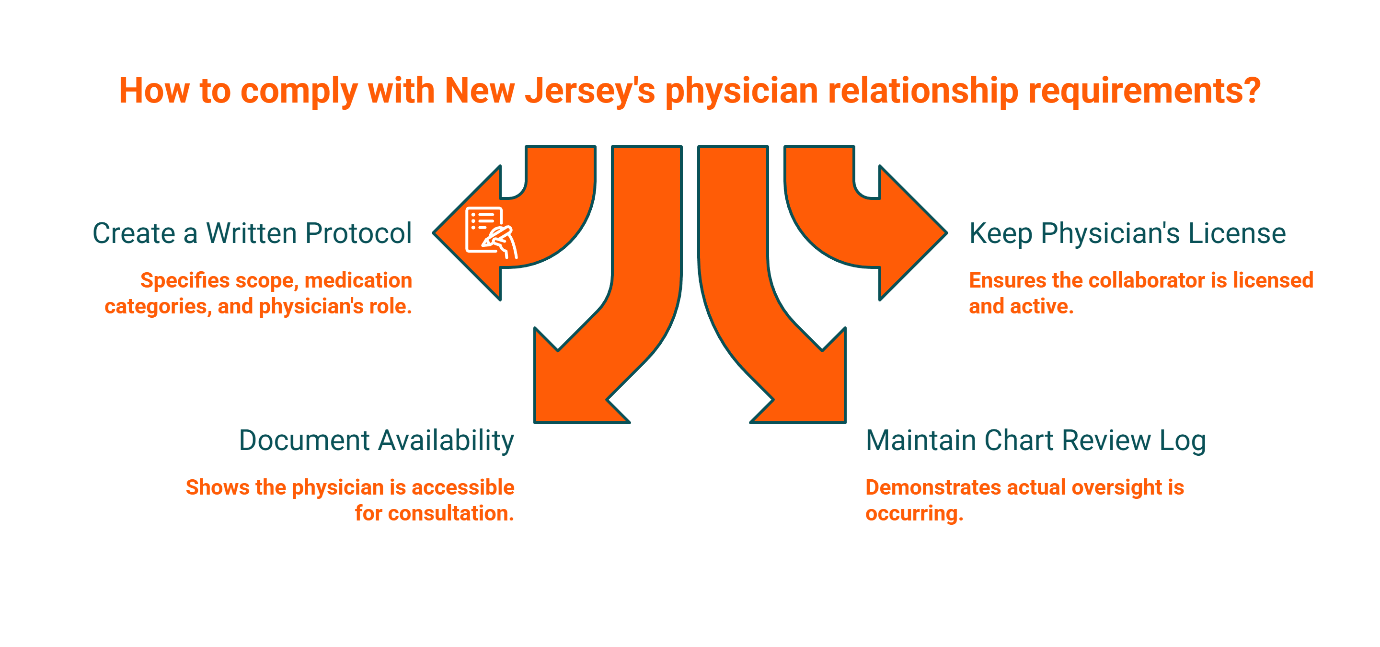
In New Jersey, the pathway to prescriptive authority for Advanced Practice Nurses is built around a formal physician-linked protocol and documentation system. If you prescribe in NJ—whether controlled substances or standard medications—you're operating under a framework that expects written protocols and a defined relationship with a supervising physician.
Here's the day-one folder you create: a written protocol document that specifies your scope, the categories of medications you'll prescribe, and the supervisory physician's role. Keep a copy of your collaborator's active NJ medical license. Document their availability for consultation (phone, secure message, scheduled check-ins). Maintain a log showing that chart reviews actually happen—not just that they're scheduled.
The trap many NPs fall into is assuming a signature alone satisfies the requirement. It doesn't. During credentialing or an audit, you need to demonstrate that the oversight relationship is functional, not theoretical.
New York: Practice Agreements vs. Modernized Pathways (What Experienced NPs Can Change)
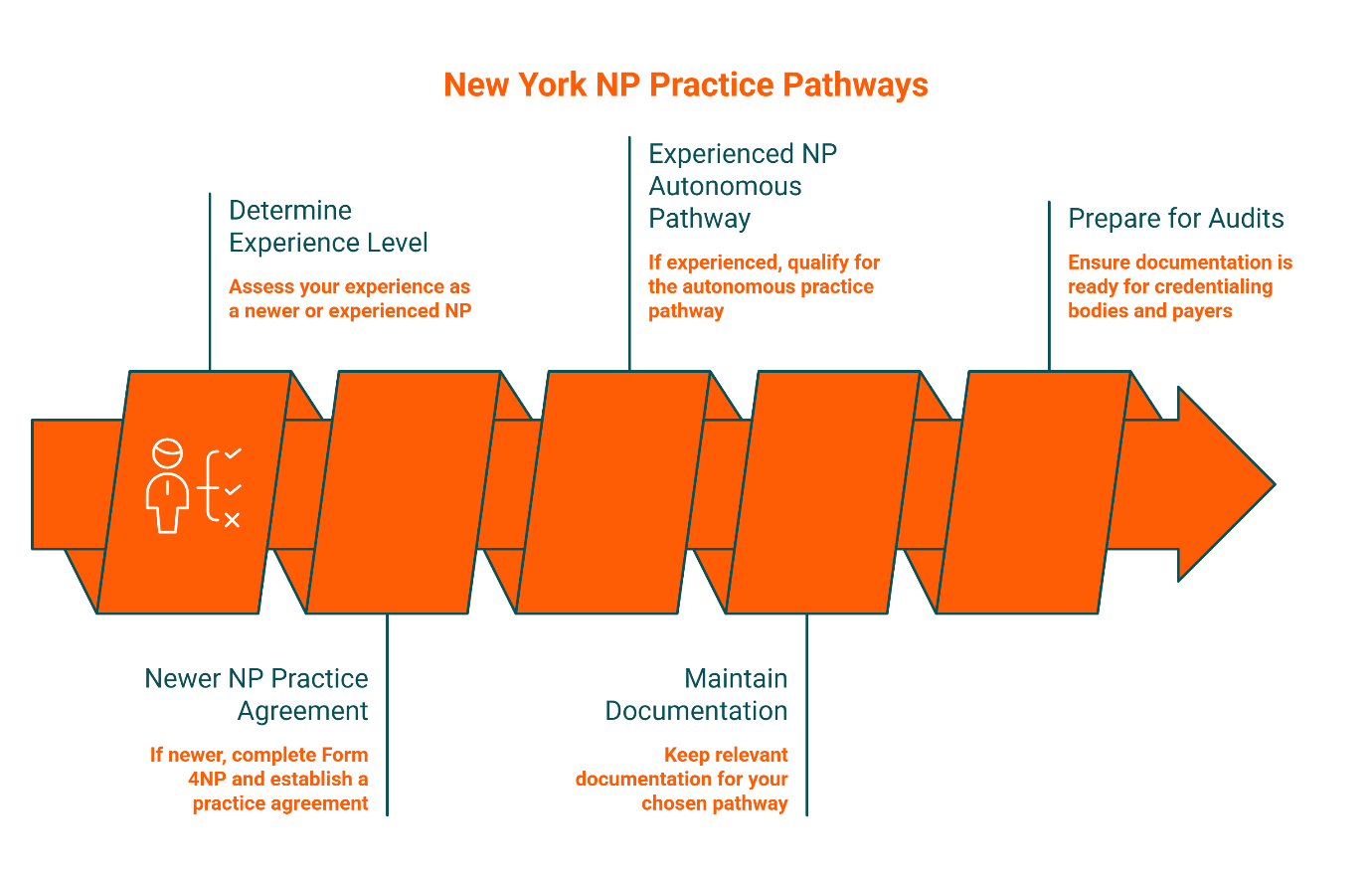
New York's framework for NP practice is defined in state education law and varies based on your experience level. If you're a newer NP, you'll typically need a written practice agreement that outlines consultation and collaboration expectations with a licensed physician. For newer NPs, this typically means completing Form 4NP, which documents the collaborative agreement and practice protocol. If you're an experienced practitioner who meets specific criteria, you may qualify for a modernized autonomous practice pathway that reduces or eliminates the need for a formal agreement.
What you keep on file depends on which pathway you're using. If you have a practice agreement, maintain a signed copy, consultation logs that prove the collaborative relationship is active, and documentation showing your collaborating physician is reachable during practice hours. The key compliance question isn't just "Do you have an agreement?" but "Can you prove consultation and review actually occurred when needed?"
For experienced NPs on the autonomous pathway, your documentation shifts to proving your qualification for that status—practice hours, certifications, and any state-mandated continuing education. Either way, credentialing bodies and payers will ask for proof. Have it ready before they ask.
Pennsylvania: Collaborative Agreement Essentials (What Must Be in Writing)
Pennsylvania operates as an agreement-forward state. The regulatory model for Certified Registered Nurse Practitioners requires a written collaborative agreement structure between the CRNP and a collaborating physician. This isn't optional, and it isn't flexible. The agreement must be in writing, signed by both parties, and specific about the scope of practice, prescriptive authority, and the nature of the collaboration.
Your minimal PA agreement checklist includes:
Scope definition: What clinical areas and patient populations you'll serve
Prescriptive authority: Clarification of what you can prescribe and under what circumstances
Chart review expectations: How often, how many charts, and what the review process looks like
Consultation availability: How you'll reach the collaborating physician when clinical questions arise
Agreement term and renewal process: Most agreements are one or two years; know your expiration date
The critical detail: your collaborating physician must hold an active Pennsylvania medical license. An out-of-state physician—even one who collaborates with you in NJ or NY—cannot serve as your PA collaborator unless they're licensed in Pennsylvania. This is a common credentialing failure point for NPs who assume one physician can cover all three states without holding tri-state licensure.
Cross-Border and Telehealth: The Rule That Prevents Accidental Non-Compliance
For telehealth, the patient's physical location typically determines which state's practice and collaboration rules apply, though this can vary depending on modality and setting. This is the single most important principle for avoiding accidental non-compliance when you're serving patients across state lines.
While state licensure relies on where the patient is located, federal DEA regulations add additional complexity to cross-state prescribing of controlled substances. If you're physically in New Jersey but conducting a telehealth visit with a patient in Pennsylvania, you're generally practicing in Pennsylvania for that encounter—and PA's collaborative agreement requirements apply. Controlled substance prescribing across state lines may involve additional federal registration requirements that go beyond state collaboration rules.
Build a routing habit to stay compliant. Your intake checklist becomes a policy:
Capture patient's physical location at the start of every telehealth encounter
Route the chart to the correct state-specific compliance folder
Verify your collaborator holds an active license in the patient's state
Document the encounter according to that state's chart review and oversight expectations
Update your malpractice carrier to confirm coverage extends to all states where you're providing telehealth services
Missing this step creates a compliance gap that won't surface until an audit, a licensing board inquiry, or a credentialing rejection. By that point, the damage is done.
How to Choose an Audit-Ready Collaborator (Without Overpaying or Gambling With Your License)
"Each state is a different world; know the rules of your territory."
The most valuable collaborator isn't necessarily the cheapest. It's the one who is reliable, reachable, and properly documented. When evaluating potential collaborating physicians or collaboration services, use these decision criteria:
State licensure match: Confirm they hold active licenses in every state where you need coverage
Documented availability: They should provide clear expectations for how and when you can reach them (not just "call if you need me")
Defensible chart review cadence: A commonly used approach is monthly reviews of a sample of your charts, though the specific frequency and percentage should align with your agreement terms and practice risk profile. Infrequent review schedules may not provide adequate oversight for active prescribing practices.
Contractual clarity: The agreement should specify what happens if the physician relationship ends unexpectedly (notice period, transition support)
Malpractice alignment: Verify their policy covers their role as your collaborator and that your policy acknowledges the collaborative structure
A "signature-only" arrangement might cost less upfront, but it increases your audit and liability risk significantly. If you can't prove oversight occurred—through review logs, consultation records, and availability documentation—you're exposed even if you have a signed agreement on file. The Board doesn't just want to see a signature; they want to see a functioning relationship.
Is a Collaboration Service a Fit for You?
Who This Is For
This model works well if you're an independent NP or PA launching or expanding a practice in New Jersey, New York, or Pennsylvania. It's especially valuable if you're running a multi-state telehealth practice and need reliable, audit-ready collaboration across all three jurisdictions without the complexity of managing multiple individual physician relationships.
Who This May Not Be a Fit For
If you're currently employed by a hospital or large practice group, your employer typically handles collaboration agreements as part of your employment structure. Students and new graduates who haven't yet started practicing independently won't need this until they're ready to launch their own practice. And if you're practicing exclusively outside the tri-state area, a service focused on NJ/NY/PA won't serve your needs.
Common Objections + Practical Answers
"Can I just pay for a signature?"
Technically, yes. Practically, no. A signature without documented oversight creates a paper shield that won't hold up in an audit. If you can't demonstrate that chart reviews happened, that your collaborator was available when needed, and that protocols were followed, the signature becomes meaningless. The cost of non-compliance—license suspension, practice shutdown, credentialing denials—far exceeds the cost of proper collaboration.
"Can one physician cover all three states?"
Only if they hold active medical licenses in New Jersey, New York, and Pennsylvania. Licensure is state-specific. A physician licensed only in NJ cannot serve as your collaborator for NY or PA patients, even if they're willing. Verify tri-state licensure before signing anything.
"What if my collaborator disappears?"
This is why contractual clarity matters. A good agreement includes a notice period (typically 30-60 days) and specifies what happens during a transition. A collaboration service mitigates this risk by maintaining a network of backup physicians and handling transitions administratively, so you're never left without coverage.
Getting Started in 3 Steps
Book a free consultation to discuss your specific practice model, patient populations, and state coverage needs
Get matched with a collaborating physician (or physicians) who hold the appropriate state licenses and specialize in your clinical area
Finalize agreements and establish your chart review workflow—typically operational within one week of signing
Your Next Step: Pick the State, Pick the Document, Pick the Oversight Routine
You now have the roadmap. New Jersey requires physician-linked protocols and documented availability. New York's requirements depend on your experience level but always demand proof that collaboration is real, not theoretical. Pennsylvania needs a written collaborative agreement structure with a PA-licensed physician and a defensible chart review process. And for telehealth, the patient's location typically drives which rulebook you follow.
The goal isn't perfection. It's preparedness. Build your compliance folders now—one per state, with the right documents, the right oversight routine, and the right proof that the relationship works—so when credentialing asks, when an audit happens, or when a licensing question arises, you're ready.
If you're practicing in New Jersey, New York, or Pennsylvania, our network of board-certified physicians understands the specific requirements of each state. Learn more about our services or review our frequently asked questions about pricing, timelines, and what's included.
Disclaimer: This content is for informational purposes only and does not constitute legal or medical advice. Requirements can vary by state and change over time. For guidance specific to your situation, consult the appropriate licensing board or a qualified professional.
Our Editorial Process:
While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.
By: About the Physician Collaborators Insights Team
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.
References:
[1] American Association of Nurse Practitioners. (2024). State Practice Environment. https://www.aanp.org/advocacy/state/state-practice-environment
[2] New Jersey Division of Consumer Affairs, Board of Nursing. Advanced Practice Nurse Requirements. https://www.njconsumeraffairs.gov/nur/Pages/APN-Certification.aspx
[3] New York State Education Department, Office of the Professions. Nurse Practitioner Practice Requirements. https://www.op.nysed.gov/professions/nurse-practitioners/professional-practice/practice-requirements
[4] New York State Education Department. Form 4NP (Collaborative Agreement & Practice Protocol). https://www.op.nysed.gov/sites/op/files/prof/nurse/np4np.pdf
[5] Pennsylvania Department of State, Bureau of Professional and Occupational Affairs. CRNP Prescriptive Authority Collaborative Agreement Requirements. https://www.pa.gov/content/dam/copapwp-pagov/en/dos/department-and-offices/bpoa/nursing/prescriptive-authority-application-process-external.pdf