
How Small NP Practices Can Prepare for Chart Review and Physician Communication Expectations
📌 Key Takeaways
A collaboration agreement only works when small NP practices turn it into a clear weekly workflow.
Workflow Comes First: Chart review works best when your team knows who prepares charts, logs feedback, and tracks deadlines.
Clarify Before Signing: Vague agreement terms can create daily problems once chart review, communication, or renewal dates begin.
Keep Records Simple: One clear folder and one naming method can make reviews easier to prove later.
Separate Communication Types: Routine questions, urgent issues, and physician feedback each need clear channels and written follow-up.
Review Before Growth: New services, telehealth, added providers, or state changes may call for another workflow check.
Clear systems protect small practices better than scattered messages and memory.
Small NP practice owners and administrators will gain practical setup clarity here, preparing them for the detailed overview that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
A signed collaboration arrangement can feel like the finish line for a small NP practice. In daily operations, it is usually the starting point.
The harder question is what happens after the agreement is in place. Which charts are reviewed? Who prepares them? How does the collaborating physician communicate feedback? Where should the practice keep review notes, communication records, and renewal reminders?
For a small NP practice with limited administrative support, those details cannot live only in memory or scattered messages. Chart review and physician communication need a workflow that your team can follow during a normal week.
Why Chart Review and Communication Need a Workflow, Not Just an Agreement
A collaboration agreement defines the relationship between a practice and its collaborating physician. The workflow determines whether that relationship is manageable in daily practice.
Chart-review timing, communication channels, documentation habits, and escalation triggers all require deliberate setup before the first review occurs. For small NP practices with limited administrative capacity, that setup matters especially—there is little margin for a process that depends on memory or informal habits. When chart review slips, when a clinical decision is discussed by text and never written down, or when an agreement renews without anyone revisiting whether the workflow still fits the practice, the consequences are operational and potentially regulatory.
The AANP classifies state NP practice environments as full practice, reduced practice, and restricted—with reduced and restricted states requiring a regulated collaborative, supervisory, or delegatory agreement as a condition of practice (American Association of Nurse Practitioners, 'State Practice Environment'). The AANP's State Practice Environment resource provides a useful national overview, and the National Council of State Boards of Nursing (NCSBN) member board profiles offer another reference point for state-specific requirements (NCSBN, 'Member Boards'). Each state board of nursing remains the legal authority on the specific rules that apply. Because collaboration requirements differ significantly by state and agreement, no single national workflow applies.
At a minimum, your practice should know:
Who prepares charts for review
How charts are selected
When review occurs
Where feedback is recorded
Which communication channels are approved
What issues require escalation
Where collaboration records are stored
Start with the Agreement Terms That Affect Daily Workflow
Before building any process, the terms that govern it need to be clearly understood—not just signed. The agreement is the starting point for every workflow decision.
The table below identifies the agreement areas most likely to shape daily operations, why each one matters operationally, and what to clarify before signing or renewing. For a deeper look at how well-constructed agreements are organized, collaborative practice agreement clauses covers essential structural considerations for independent NPs.
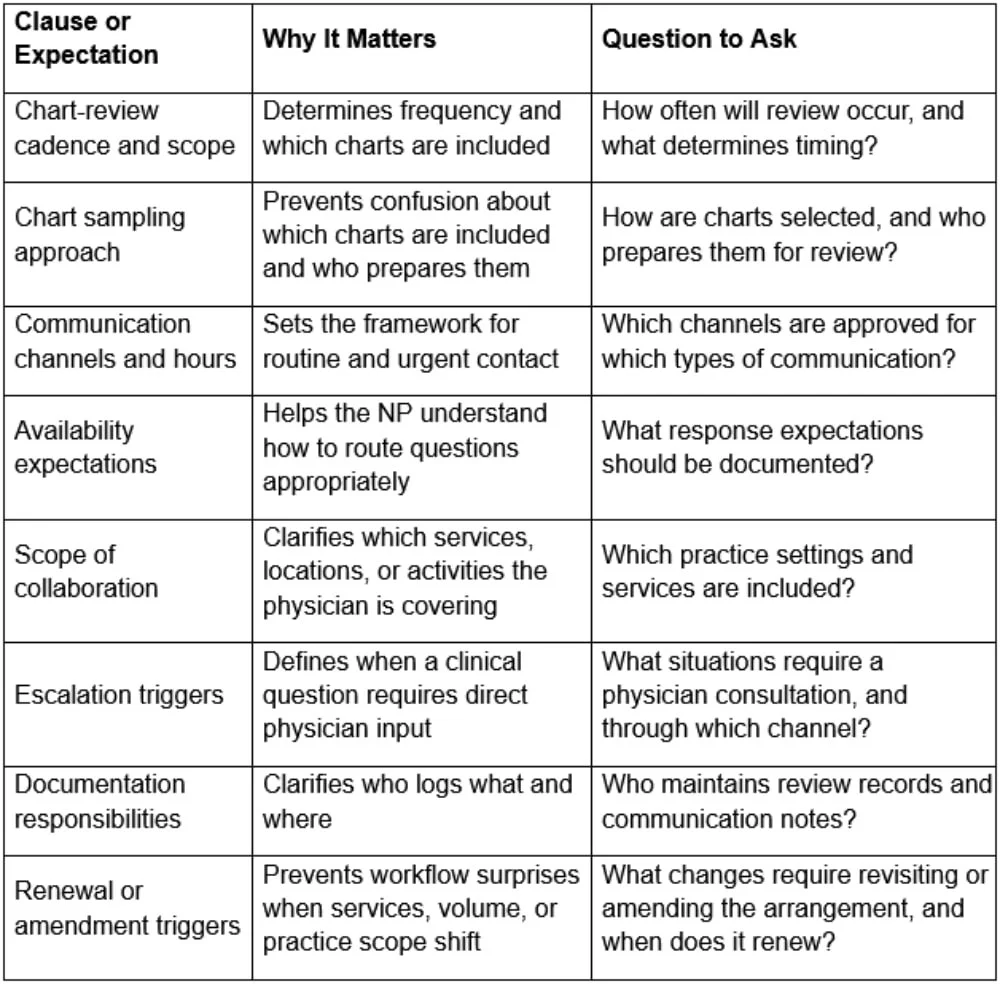
If any item in that table cannot be answered clearly from the current agreement, clarify it before the arrangement is operational. Vague language becomes a process problem the moment the first review is scheduled.
A useful test: if a new administrator joined your practice tomorrow, could they understand how chart review and physician communication are supposed to work? If not, the workflow needs more clarity before the arrangement becomes part of daily operations.
Build a Chart-Review Process Your Team Can Actually Maintain
Chart review requires an internal owner to stay consistent. The practice is responsible for preparing charts, confirming the schedule, and documenting each outcome—it is not a task the collaborating physician manages unilaterally.
For example, if a small primary care NP practice starts a collaboration arrangement without designating a review coordinator. Reviews drift later each month because nobody owns the task. Physician feedback is discussed informally and never logged. By renewal time, there is no record showing what was reviewed or when. A modest amount of process clarity at the outset prevents that outcome entirely.
A workable process for most small practices follows five steps.
First, confirm the review cadence and scope based on your agreement and applicable requirements. Some states specify minimums; others leave the cadence to the agreement. Avoid assuming one frequency applies everywhere.
Second, decide who prepares charts for review. In a small practice, this may be the NP owner, a practice administrator, or another assigned team member. The role does not need to be elaborate—it needs to be explicit.
Third, document how charts are selected. The method should match the agreement and any applicable rules. Whether charts are chosen randomly, by condition, or by volume depends on agreement terms and state requirements. Confirming the method before using it avoids a process dispute later.
Fourth, create a review log. The log may track the review date, chart identifier, reviewer, feedback status, and follow-up owner. Keep it practical and avoid placing unnecessary sensitive patient information in general administrative logs.
Fifth, schedule review reminders. A calendar reminder—not an informal intention—keeps the review on track. Physician Collaborators' FAQ describes collaboration as including physician review of a sample of charts each month. Logging when that review happened, what was covered, and what follow-up was needed is the practice's responsibility, not the physician's alone.
Define Communication Expectations Before Questions Become Urgent
Informal communication habits create ambiguity at exactly the moments when clarity matters most: an urgent question that waits hours, a care decision made verbally and never documented, a concern escalated through a channel nobody agreed to use.
The most practical communication workflows separate four categories: routine administrative questions, scheduled chart-review feedback, time-sensitive clinical or operational questions, and escalation issues. Each category should not rely on the same informal process.
Physician Collaborators' FAQ describes collaboration as including access to the physician via encrypted text message, phone call, or email during regular business hours, with Zoom conferences available for more hands-on guidance. How any specific arrangement handles communication—channels, availability windows, escalation paths—should be confirmed in the agreement or directly with the provider.
Worth clarifying before the arrangement becomes active:
Which channels are appropriate for routine versus time-sensitive questions?
What is the expected response window for non-urgent matters?
Who on the practice team is authorized to contact the physician?
How will communication involving a clinical or operational decision be documented?
Before relying on any channel for clinical communication, confirm it meets the privacy and documentation standards applicable to the practice. The U.S. Department of Health and Human Services provides HIPAA guidance materials and an overview of the HIPAA Security Rule, but your practice should confirm how those obligations apply to its own systems and workflows. Suitability depends on agreement terms and applicable requirements—not on convenience.
A communication log does not need sophisticated tools. A consistent record of who was contacted, when, about what, and what was decided is more useful than an elaborate system nobody maintains. The practical rule: routine questions need a channel, but important decisions need a record.
Keep Collaboration Records Organized Without Overbuilding the System
Documentation habits become the system when a small practice has no dedicated compliance staff. Records that need to be produced under pressure are rarely compiled quickly if they were never organized to begin with.
Core records worth maintaining in one consistent, accessible location include the current agreement and any amendments, chart-review logs with dates, scope, feedback, and follow-up actions, notes from communication involving clinical or operational decisions, records of scheduled consultations, and the agreement renewal date with a workflow review scheduled beforehand.
One folder and one naming convention serve most small practices adequately. A simple file structure might include:
Collaboration Agreement – Current
Chart Review Log – 2026
Communication Notes – 2026
Amendments and Updates
Renewal Review Notes
Provider Contact and Escalation Process
The goal is a record that shows when reviews occurred, what was discussed, and whether follow-up happened—without requiring reconstruction later. Sensitive patient details belong in the clinical record, not in general collaboration logs. For context on the documented risks of relying on informal supervisory agreements without adequate structure, that topic is addressed in a dedicated resource on the hidden financial and legal risks of informal supervisory agreements.
Chart Review and Communication Readiness Checklist
An operational preparation tool. Requirements vary by state and agreement.
[ ] Agreement terms reviewed and clarified before signing or renewing
[ ] Chart-review cadence and scope confirmed as consistent with agreement terms and applicable requirements
[ ] Chart selection process documented
[ ] Internal owner assigned for preparing charts, scheduling reviews, and logging outcomes
[ ] Review window added to the practice calendar
[ ] Review log created and stored consistently
[ ] Approved communication channels confirmed with the physician
[ ] Routine and time-sensitive communication processes separated
[ ] Escalation triggers defined and documented
[ ] Communication log process in place and accessible to responsible staff
[ ] Follow-up owner assigned after physician feedback
[ ] Records stored in a single, consistently named location
[ ] Renewal date on the calendar with a workflow review scheduled beforehand
[ ] Workflow review planned for service changes, telehealth expansion, new states, or major volume changes
[ ] State-specific and agreement-specific requirements verified through official sources or qualified professional guidance
Use the checklist to prepare targeted questions before speaking with a collaboration provider.
Review the Workflow Before Renewal, Expansion, or Service Changes
Collaboration readiness is not a one-time setup task. A process suited to a small practice at launch may not fit the same practice after it adds telehealth, expands prescribing scope, brings on a second provider, or sees meaningfully different patient volume. Treat every renewal as a workflow review, not simply a re-signing.
Confirm that the review cadence still reflects current volume, that the communication process still matches how the team actually works, and that the physician's specialty still aligns with the services being delivered. Practice changes that commonly warrant a workflow and agreement review include adding telehealth delivery, expanding into controlled-substance prescribing, changing states of practice, and bringing in additional providers.
As the AANP notes, each state board of nursing is the legal authority on specific requirements—verify amendment or renewal triggers through official channels before assuming the existing arrangement still applies.
For a broader overview of how collaboration requirements differ by state, restricted vs. reduced practice states offers useful context.
Questions to Ask a Collaboration Service Provider
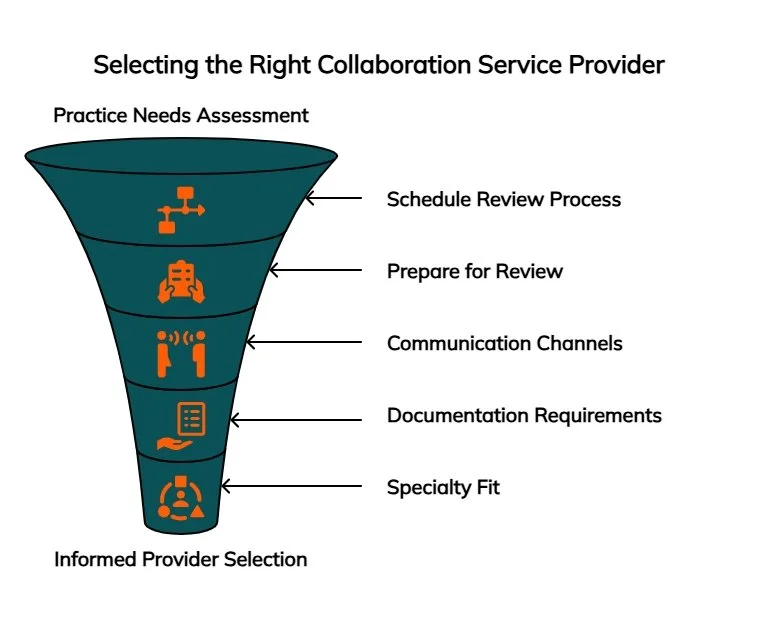
A clearer picture of the practice's chart-review and communication needs should drive the questions brought to any collaboration service. The right collaborating physician fits the practice's actual workflow, specialty, and communication expectations—not simply a general category of availability.
Useful questions for any provider evaluation:
How is chart review scheduled, and who initiates the process?
What does the practice need to prepare before review?
Which communication channels are available for routine and urgent questions?
What documentation does the practice need to maintain, and what does the provider expect?
How is specialty fit assessed, and what happens when services or volume change?
How are state-specific requirements handled for telehealth or multi-state practices?
What should be reviewed before renewal?
Physician Collaborators is a network of board-certified physicians with experience collaborating with NPs and PAs across a range of practice types, including general medicine, behavioral health, telemedicine, urgent care, infusion therapy, integrative medicine, and med spa. If there is uncertainty about whether a situation calls for a collaborating physician or a medical director, medical director vs. collaborating physician explains what each role actually covers.
Frequently Asked Questions
How often should an NP practice complete chart review with a collaborating physician?
There is no nationally uniform answer. Frequency depends on state requirements, the specific agreement terms, and practice context. Some states specify minimums; others leave the cadence to the agreement. Before assuming any frequency is sufficient, verify current requirements through the relevant state board or a qualified professional familiar with NP practice in that state.
What should be documented after a chart review?
Generally, practices may track the review date, a chart identifier consistent with applicable privacy standards, the reviewer's name, feedback received, and any follow-up actions. Consistency matters more than format—incomplete or informal records are harder to rely on and harder to reconstruct. Specific recordkeeping requirements should be confirmed with qualified professional guidance.
What communication expectations should be clarified with a collaborating physician?
At minimum: which channels are approved for routine and urgent questions, available hours and expected response windows, which situations require direct physician input, how communication involving clinical decisions will be documented, and who on the practice team is authorized to make contact.
Can informal communication with a collaborating physician create documentation problems?
It can introduce significant ambiguity. When clinical or operational decisions are discussed verbally or through untracked channels, there is no record of what was agreed to or followed up on. That matters during agreement reviews and any external review of practice operations. Establishing a documentation standard before it is needed is far simpler than defending gaps afterward.
Should a collaboration agreement be reviewed by a professional before signing or renewing?
For arrangements involving state-specific legal obligations, prescriptive protocols, chart-review requirements, or other compliance-sensitive terms, consultation with a qualified legal or compliance professional familiar with NP practice in the relevant state is strongly advisable. General educational content does not substitute for that review.
Prepare the Workflow Before You Need to Prove It
Chart review and physician communication expectations work best when they are clarified early. A collaboration arrangement functions most reliably when the processes around it are clearly defined before the first review is due, the first urgent question arrives, or an agreement renewal approaches unannounced.
Small NP practices are often well-positioned to build these workflows efficiently—fewer stakeholders, more direct ownership of each step, and a clearer picture of what the team can realistically maintain. The goal is not a heavy compliance system; it is a repeatable one.
Start with the agreement. Turn key expectations into calendar reminders, review logs, communication rules, and renewal questions. Keep the process simple enough for your team to maintain during a normal week. Use the checklist above to prepare targeted questions before speaking with a collaboration provider. For state-specific obligations, agreement clause language, or documentation requirements, verify current requirements through the appropriate board or a qualified professional.
To discuss specific practice needs or explore collaboration support options, contact Physician Collaborators for a free quote.
Disclaimer: This article is for general informational purposes only and does not constitute compliance, legal, medical, or professional advice. Collaboration, chart-review, communication, and documentation requirements may vary by state, agreement, practice type, and regulatory context. Confirm important decisions with the appropriate board, qualified legal or compliance professional, and licensed healthcare professionals involved in your practice.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the Physician Collaborators Insights Team:
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice. This guide is intended as a comprehensive starting professional.