
Documentation Gaps That Can Complicate NP-Physician Collaboration Compliance
📌 Key Takeaways
A signed agreement is only the start; practices also need records that show how NP-physician collaboration works.
Match Paper To Practice: Review the agreement against real services, prescribing, telehealth, and daily work.
Record Chart Reviews: Keep simple logs showing review dates, reviewers, sampled charts, feedback, and follow-up.
Define Communication Rules: Set clear channels for routine questions, urgent issues, and expected response times.
Separate Key Roles: Clarify what the NP, physician, practice, and medical director each handle.
Track Every Change: Update files when services, states, physicians, prescribing scope, or renewal dates change.
Good collaboration is easier to defend when the paperwork matches the work.
NP practices and healthcare teams will gain a clear readiness check here, preparing them for the detailed overview that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
A practice may have a signed collaboration agreement on file and still carry documentation gaps that create friction exactly when they matter most—during renewal, a board inquiry, a payer question, or the transition to a new collaborating physician. The signed agreement is an important foundation, but it is typically one part of what documents an arrangement. Supporting records that show how the collaboration actually functions are where gaps most commonly appear, and requirements for what those records should include vary meaningfully by state, practice type, and agreement terms. The five sections below address the most common gap areas, followed by a readiness checklist to use before signing, renewing, or evaluating an existing arrangement.
Note: This article addresses documentation readiness, not legal advice. Requirements vary by state and agreement. Confirm current rules with the relevant licensing board, a qualified attorney, or a compliance advisor.
Why Documentation Gaps Matter Even When an Agreement Is Signed
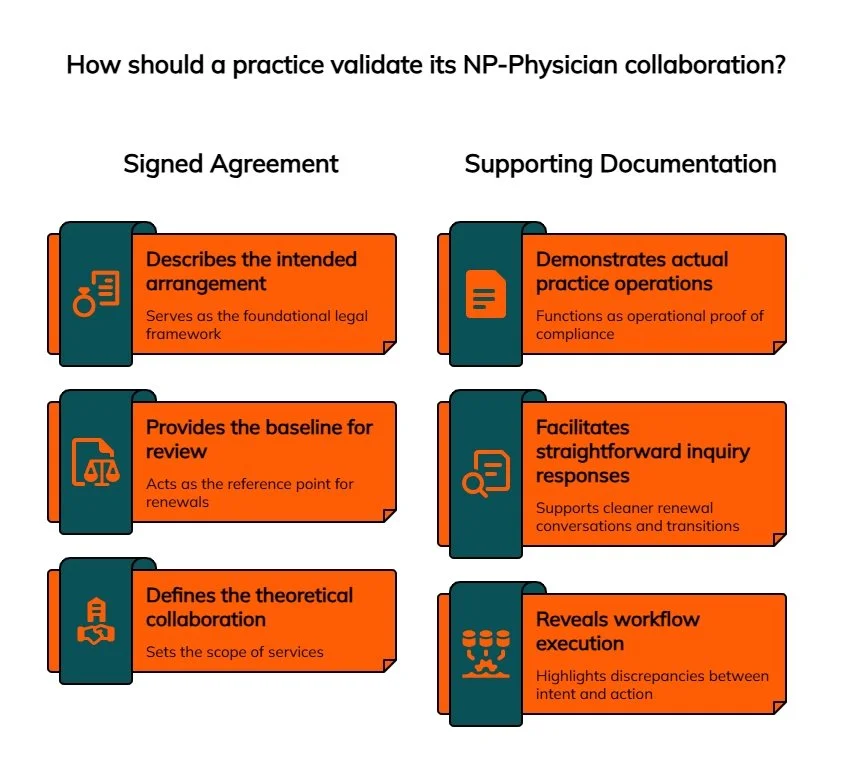
The signed agreement describes an arrangement. Supporting documentation shows whether the practice is actually running the one it signed—and those two things are not always the same.
Gaps tend to surface at moments of transition or scrutiny: a renewal that requires reviewing the original document, a practice expansion that forces a look at whether current services still fall within the agreement's scope, or a physician change that raises questions about what records exist. A practice may find it can describe the collaboration clearly but cannot demonstrate it through written records. That distinction matters because documentation functions as operational proof. Whether state rules address it explicitly—and to what degree—varies considerably. Regardless, organized documentation supports cleaner renewal conversations, smoother transitions, and more straightforward responses to any inquiry.
The American Association of Nurse Practitioners' State Practice Environment resource is a useful starting point for understanding that NP practice authority differs across jurisdictions, and the National Council of State Boards of Nursing provides broader APRN regulatory context through its APRN Consensus Model.
A pragmatic documentation-readiness file should help the practice answer three questions: What does the agreement say? What does the workflow actually do? What needs state-specific or professional review? The goal is not to document everything—it is to make the collaboration arrangement clear, current, and easier to review.
Gap 1: Agreement Clauses That Do Not Match the Real Workflow
The most common documentation gap starts with an agreement that was accurate at signing but has not been revisited since. Practices evolve—services change, telehealth gets added, prescribing scope shifts—while the agreement stays fixed.
Before evaluating clause language, a useful first question is whether the agreement clearly identifies who is collaborating with whom. The specific NP or NPs and the specific physician should be named, and the scope should be defined clearly enough that both parties can determine whether a given clinical situation falls within it. Several clause areas frequently reveal a gap between what the document says and what the practice does:
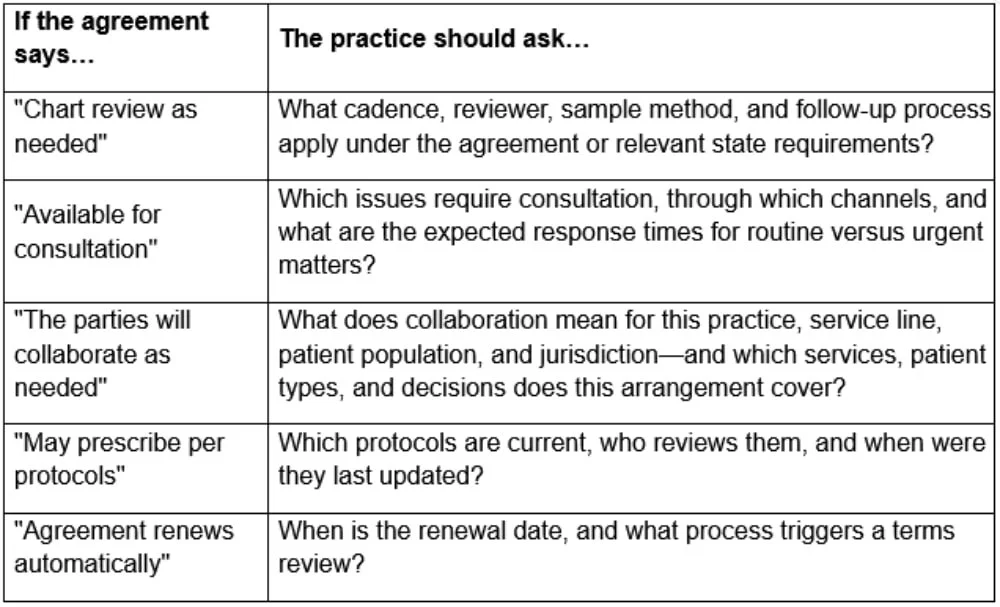
Identifying these gaps often begins by comparing what the agreement says to what the practice does. Required agreement clauses may vary by state; current state board materials, statutes, regulations, or qualified legal and compliance review should be used before treating any clause as mandatory. For a closer look at the clauses collaborative practice agreements commonly need to address, this post on collaborative practice agreement clauses provides useful context.
Gap 2: Chart Review Expectations Without Review Records
Chart review is one of the most tangible elements of an active collaboration arrangement—and among the most consistently underdocumented. A practice might follow a consistent monthly review cadence but keep no record of which charts were reviewed, what feedback was provided, or whether follow-up occurred. The review happened, but demonstrating it would require reconstructing information from memory rather than referencing a log.
Useful documentation does not need to be elaborate: a note capturing the review date, the reviewer, the charts sampled, and any resulting discussion typically establishes that the process is active. Where the agreement specifies a frequency or format, records should reflect it. Physician Collaborators describes its collaboration model as including monthly sample chart review alongside access via text, email, phone, or video conference—one example of what a structured arrangement can look like operationally. Chart review requirements vary by state and agreement; a practice should verify current standards with the appropriate board or a qualified advisor rather than assuming any single rule applies.
A critical operational distinction: a chart review record may identify the review process without duplicating unnecessary patient details in informal logs. The record should help show that review occurred and that follow-up was handled when appropriate. This distinction matters because what belongs in a patient record, what belongs in a collaboration log, and what should not be duplicated outside secure systems are three separate decisions—and leaving them unresolved is itself a documentation gap.
This is especially relevant when review is informal. A quick conversation with a collaborating physician may be clinically useful, but the practice still needs to determine what gets formally recorded and where. Review that cannot be located or explained is difficult to rely on during renewal or transition, even when the underlying collaboration has been active and attentive.
Gap 3: Informal Communication Without Clear Channels or Escalation Notes
Most collaboration communication happens informally—texts, calls, email threads—without written expectations around any of it. The gap here is not about volume. It is about whether shared expectations exist and can be referenced.
Consider a hypothetical practice where urgent clinical questions and routine administrative ones arrive through the same text thread to the collaborating physician. Without a defined escalation pathway, there is no shared framework for knowing which messages need prompt clinical attention and which can wait—and both parties may hold entirely different assumptions with nothing to resolve the discrepancy.
A brief written description of which channel handles routine matters, which handles urgent escalation, and what response windows apply creates that shared reference. Documenting significant clinical decisions that arise through collaboration—when a case was escalated, what guidance was provided, what outcome followed—also creates a meaningful operational record rather than simply evidence that the arrangement exists.
Any communication involving patient information should comply with the practice's privacy and security obligations. The HHS Office for Civil Rights maintains current HIPAA guidance applicable to healthcare communication settings, but specific implementation decisions should be reviewed with a qualified privacy or compliance professional.
Gap 4: Unclear Role Boundaries Between the NP, Physician, and Practice
Role terminology carries operational weight that is easy to underestimate. "Collaborating physician," "supervising physician," "medical director," and "consulting physician" can carry meaningfully different legal and operational meanings depending on the state, the arrangement, and the payer context—yet practices sometimes use them interchangeably in billing documentation and internal communications without defining what each covers.
A common hypothetical: a practice uses "collaborating physician" and "medical director" interchangeably in billing paperwork, and when a payer audit asks for documentation of the medical director's responsibilities, no clear record exists.
To prevent that kind of ambiguity, the documentation should clarify who owns each part of the collaboration workflow. That may include:
Keeping the current signed agreement accessible and clearly labeled
Tracking chart review completion and storing review logs
Documenting consultation or escalation outcomes
Updating workflow documents after service changes
Reviewing physician licensure or specialty fit when relevant
Flagging issues for attorney, board, or compliance-advisor review
This is not only a legal distinction—it is a workflow-control issue. If nobody owns chart review records, renewal reminders, or agreement version control, the documentation file can become outdated even when the collaboration relationship is active. Where a practice has both a collaborating physician and a separate medical director, keeping their responsibilities clearly delineated matters for billing accuracy and regulatory clarity alike. For a practical overview of how these roles differ, this post on the medical director vs. collaborating physician distinction is a useful reference. State-specific definitions require verification through current official sources.
Gap 5: Renewal, Scope Changes, and Version Control That Are Not Tracked
Collaboration documentation becomes outdated without either party noticing—and when it does, the misalignment tends to surface under exactly the conditions when accuracy matters most. The correction is not to define a universal renewal frequency, but to establish clear review triggers and verify any state-specific timing requirements.
A practice that added telehealth services after the agreement was originally signed may be operating every virtual encounter under a document that does not describe it—a gap that only becomes apparent under scrutiny. Several circumstances commonly warrant a documentation review: adding or removing a service line, expanding telehealth into new states, adjusting prescribing or controlled-substance scope, and approaching a renewal date are the expected triggers. A change in the existing collaborating physician's availability—reduced hours, an adjusted response channel, or a coverage gap that was never formally addressed—is a less obvious but real trigger, since the current arrangement may no longer accurately reflect operating terms.
Version control is a straightforward gap to close. If an agreement was amended through an email or a verbal discussion without the main document being revised and re-signed, neither party has a reliable current record. Maintaining a log of the current signed version and any subsequent amendments, with dates, prevents the confusion that arises when parties later disagree about what was agreed to. For practices with multi-state telehealth operations, the post on being a telehealth-ready collaborator covers cross-state compliance considerations in more detail.
A Practical Documentation Readiness Checklist Before Signing or Renewing
Use this as a readiness review prompt, not a legal compliance checklist. Whether any item is legally required depends on the state, agreement, and current regulations. Use it to organize a documentation review and prepare questions for qualified review.
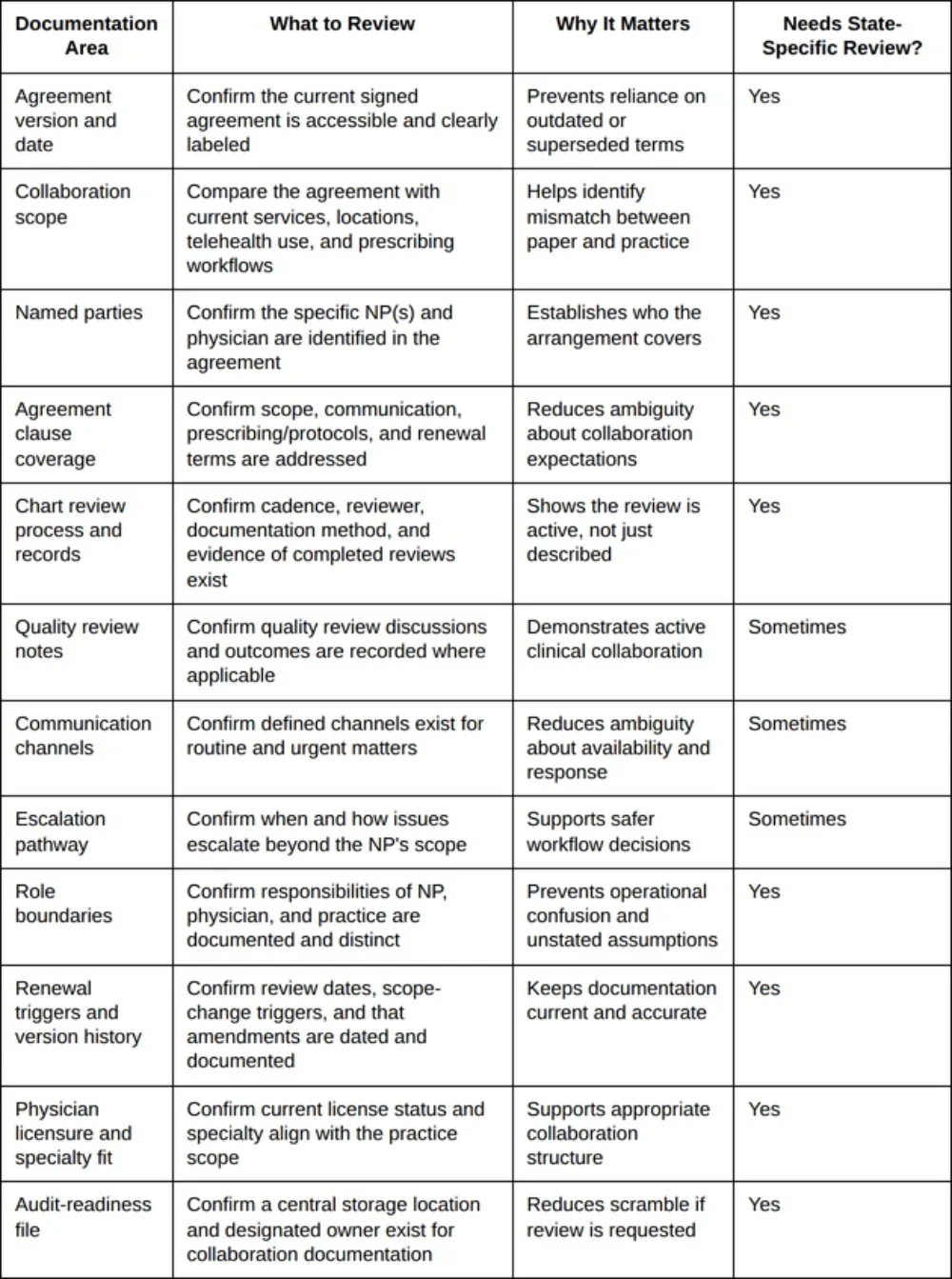
Use this checklist to prepare questions for an attorney, compliance advisor, or collaborating physician support provider—not as a substitute for qualified professional review. The most useful version of this checklist is specific to the practice: a med spa, behavioral health practice, urgent care setting, telehealth practice, and general medicine practice may not have the same collaboration workflow. The review process should reflect the actual practice model.
When to Bring in Legal, Compliance, or Collaboration Support

The documentation areas above are a starting point for identifying where records may be unclear, incomplete, or out of date. For questions about what is legally required in a specific state—which clauses must appear, what chart review standards apply, whether filing or renewal processes are mandated—qualified legal or compliance review is the appropriate resource. The National Council of State Boards of Nursing maintains APRN practice authority and regulatory resources that can help orient a research process, though state-specific requirements should always be confirmed through official state sources or qualified counsel.
Documentation review is most manageable at predictable checkpoints rather than in response to an inquiry: before signing a new agreement, at renewal, when expanding services or telehealth states, and when transitioning to a new collaborating physician. A collaboration support provider can help structure the operational side of an arrangement—physician matching, chart review workflows, communication expectations—but cannot replace the legal or compliance review that state-specific requirements may call for. For background on how collaboration requirements differ across practice authority categories, the post on restricted vs. reduced practice states provides useful context. If your practice is evaluating or establishing a collaboration arrangement, Physician Collaborators connects advanced practice providers with board-certified physicians and psychiatrists across multiple practice types—contact the team for a free quote.
Staying Ahead of Documentation Gaps
Compliance readiness in NP-physician collaboration involves more than a signed agreement. The supporting records—documented chart reviews, defined communication expectations, clear role boundaries, tracked renewal triggers, and version-controlled agreements—give the arrangement its operational structure.
The five gaps covered here are manageable when identified before renewal, expansion, physician transition, or a compliance review, and considerably harder to address during one. Documentation gaps are easiest to close at predictable checkpoints: before signing, at renewal, when expanding services or telehealth states, and when the practice changes physicians. Starting by organizing the current file, identifying what is unclear, and flagging state-specific questions for a qualified professional makes that process significantly more straightforward. The readiness checklist above is a practical starting point for that work. To explore physician matching and collaboration support structures, contact Physician Collaborators for a free quote.
Frequently Asked Questions
Is a signed collaboration agreement enough for compliance?
Not necessarily. A signed agreement may be important, but practices may also need supporting records that show how collaboration, chart review, communication, renewal, and role boundaries work in practice. Requirements can vary by state, agreement terms, and practice type. Confirming current expectations with the relevant board or a qualified advisor is an important step before relying on the agreement alone.
What documentation should an NP practice review before renewing a collaboration agreement?
Renewal is a useful checkpoint for the full documentation picture: the current signed version, chart review process and records, communication channel expectations, escalation pathways, role boundaries, renewal triggers, physician availability, and any state-specific requirements that may have changed since the original signing. The checklist above provides a structured starting point.
Do chart review documentation requirements vary by state?
Yes. Chart review frequency, format, and required scope can differ across state statutes, board rules, and individual agreement terms. A practice should verify current requirements through its state board of nursing, state medical board, or qualified counsel rather than assuming one standard applies universally. The National Council of State Boards of Nursing provides a useful orientation to APRN regulatory frameworks, though state-specific rules require direct verification through official sources.
Who should review collaboration documentation?
Depending on the practice, the NP owner, compliance lead, administrative staff, collaborating physician, attorney, and compliance advisor may each have a role. The important point is to assign ownership so that records do not remain scattered across systems and inboxes. When nobody owns a documentation area—chart review logs, renewal tracking, version control—gaps tend to persist regardless of how active the underlying collaboration is.
When should a collaboration agreement be updated?
An agreement may warrant review when the practice changes services, adds a location, expands telehealth into new states, changes collaborating physicians, adjusts prescribing scope, or approaches a renewal date. A change in the existing physician's availability—reduced hours or adjusted communication channels—is also worth noting, since it may affect whether the agreement accurately reflects the current arrangement.
Disclaimer: This article is for general informational purposes only and does not constitute legal, medical, compliance, safety, or professional advice. Requirements and documentation expectations may vary by state, practice type, agreement terms, and current regulations. Confirm important decisions with the relevant licensing board, qualified attorney, compliance advisor, or other appropriate professional.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the Physician Collaborators Insights Team:
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.