
Restricted vs. Reduced Practice States: How Your Location Impacts Collaboration Requirements
📌 Key Takeaways
Where you practice determines whether you need a collaborating physician—and for how long.
State Category Sets the Rules: "Full," "reduced," or "restricted" tells you if collaboration is required, but each state's specific paperwork and oversight rules vary.
"Reduced" Doesn't Mean Temporary: States like New Jersey and Pennsylvania require ongoing collaboration that never phases out, even with years of experience.
New York Uses an Hours Threshold: NPs with fewer than 3,600 qualifying hours must have a written agreement; after that, they can practice independently.
Moving States Can Reset Your Requirements: A practice model that works in one state may require a collaborating physician the moment you treat patients elsewhere.
Always Verify Before You Launch: Start with the AANP map, then confirm the current rules directly with your state board before opening or expanding.
Know your state category first—then check the fine print before you sign a lease.
Nurse practitioners planning independent or multi-state practices will clarify their collaboration requirements here, preparing them for the detailed state-by-state breakdown that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
The state where you practice determines whether you need a collaborating physician, how long that arrangement must last, and what oversight looks like day to day. Understanding the difference between restricted and reduced practice states is the first step toward building a compliant independent practice.
Restricted vs. Reduced Practice States: The Fast Answer
Nurse practitioner practice authority falls into three categories defined by the American Association of Nurse Practitioners (AANP): full practice, reduced practice, and restricted practice. In full practice states, NPs can evaluate, diagnose, order tests, and manage treatment under exclusive board-of-nursing authority without physician involvement. Reduced practice states limit at least one element of NP practice and may require a collaborative agreement or impose setting restrictions. Restricted practice states require career-long supervision, delegation, or team management by another health provider for at least one element of care.
State category tells you the level of independence; state-specific rules tell you the exact paperwork and collaboration burden.
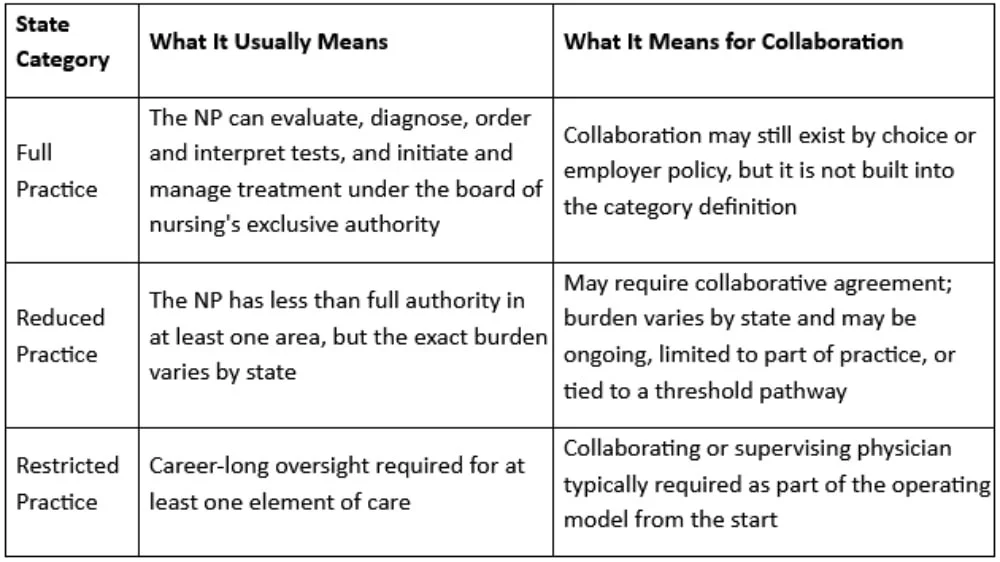
Think of the category as the map, not the trip. It tells you whether a state is broadly full, reduced, or restricted—but not the specific paperwork, protocols, or chart review requirements. That is why the safe next move is always to confirm the live rule with the relevant board or office of professions.
What a Restricted Practice State Means for an NP
Restricted practice states require physician oversight for at least one element of NP practice throughout your entire career. This is not a temporary arrangement or a transition period you can work through. The oversight requirement is baked into state law.
Geography determines autonomy. A practice plan that works cleanly in one state can become non-compliant after a move, a second-state expansion, or a shift into a different care setting.
For practice owners, this has immediate operational implications. Launch planning must include securing a collaborating or supervising physician before you can see patients. Prescriptive authority workflows often require physician involvement. Your entire practice model depends on maintaining this relationship, which means building contingency plans for physician availability and considering what happens if that relationship ends.
The risk of operating without proper oversight in a restricted state is not abstract. It can affect licensure, prescribing privileges, and payer enrollment. Understanding that your state falls into this category should prompt a clear next step: confirm the exact oversight structure your board requires and understand what a collaborative practice agreement actually covers.
What a Reduced Practice State Means for an NP
Reduced practice sits between full independence and restricted practice, but the exact burden varies significantly from state to state. Some states use threshold-based pathways where collaboration requirements phase out after you accumulate enough experience. Others maintain ongoing collaborative or written-agreement requirements for specific elements of practice, such as prescribing.
This variation matters. Assuming all reduced-practice states work the same way can lead to costly compliance mistakes.
Why "Reduced" Does Not Always Mean "Temporary"
New Jersey and Pennsylvania both carry a reduced-practice classification, but neither offers a simple transition to independence.
According to the New Jersey AANP fact sheet, APNs must maintain joint protocols with a collaborating physician to order medications and devices. New Jersey board materials also tie prescriptive authority to a joint protocol with a collaborating physician licensed in New Jersey. This is not a transition period—it is an ongoing requirement tied to prescriptive practice.
The Pennsylvania AANP fact sheet similarly classifies the state as reduced practice and states that NPs must have a career-long written agreement with one or more physicians. Pennsylvania adds prescriptive-authority collaboration requirements for NPs with current prescriptive authority approval.
The lesson is straightforward: reduced practice is a category, not a promise of eventual full autonomy. Always verify the specific rules in your state before assuming your collaboration requirement will sunset. Relying on informal assumptions about how these arrangements work creates real financial and legal exposure.
New York as the Clearest Transition-Style Example
New York offers the clearest example of a threshold-based pathway within the reduced-practice category. According to the New York Office of the Professions, NPs must practice with written practice protocols and a written practice agreement with a collaborating physician unless or until they complete more than 3,600 hours of qualifying NP experience. Once that threshold is crossed, New York does not require physician supervision or chart co-signature, and NPs may practice independently.
This model rewards experience with greater independence. But it still means newer NPs in New York need a collaboration arrangement in place to practice compliantly during their early career years.
Why Your State Category Changes Your Collaboration Plan
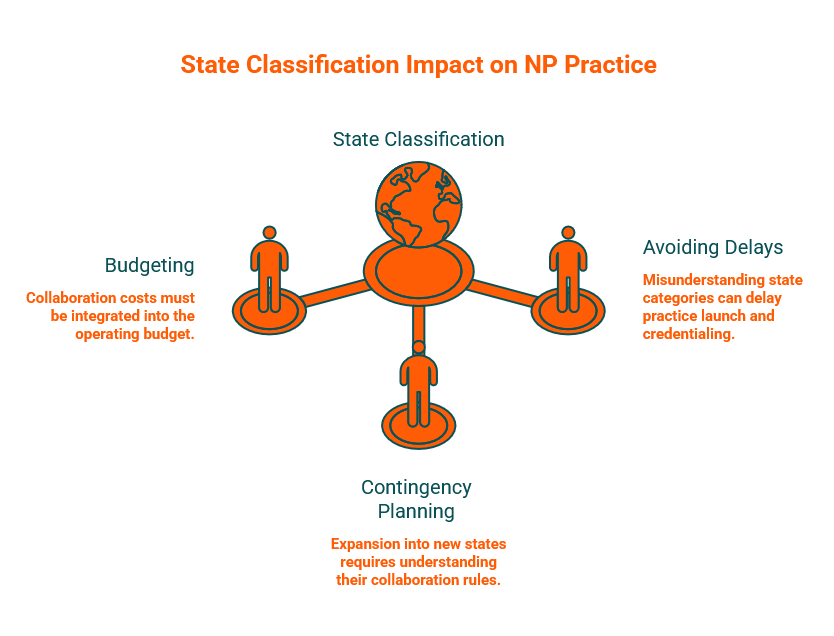
Your state's classification shapes several operational decisions that affect your bottom line and your ability to launch or grow.
Budgeting: If your state requires current collaboration, that cost must be part of your operating budget from day one. Collaboration arrangements typically involve monthly fees, and the right partner also provides clinical support and compliance documentation.
Contingency planning: If you are considering expanding into additional states—especially through telehealth across state lines—you need to understand how each new state's classification changes your requirements. A practice model that works in a full-practice state may require a collaborating physician the moment you treat a patient in a reduced or restricted state.
Avoiding delays: Misunderstanding your state's category can delay practice launch, credentialing, or payer enrollment. Payers and credentialing bodies expect documentation that you are practicing within your legal scope—which may include proof of a valid collaboration arrangement.
Real-World Examples: New York, New Jersey, and Pennsylvania
The tri-state region illustrates how different reduced-practice implementations create different collaboration burdens. For a deeper breakdown, see The NJ/NY/PA Protocol.
New York
New York requires a written practice agreement with a collaborating physician for NPs with fewer than 3,600 hours of qualifying experience. Once that threshold is met, the agreement is no longer required. New York does not require physician supervision or chart co-signature for experienced NPs, and those with more than 3,600 qualifying hours may practice independently.
New Jersey
New Jersey maintains a reduced-practice classification. APNs must have joint protocols with a collaborating physician for prescribing and ordering medications and devices. New Jersey board materials tie prescriptive authority to a joint protocol with a collaborating physician licensed in New Jersey. This requirement does not phase out with experience.
Pennsylvania
Pennsylvania also carries a reduced-practice classification. NPs must maintain a career-long written collaborative agreement with one or more physicians. The state adds prescriptive-authority collaboration requirements for NPs with current prescriptive authority approval.
How to Verify Your State's Current Rules Before You Open or Move a Practice
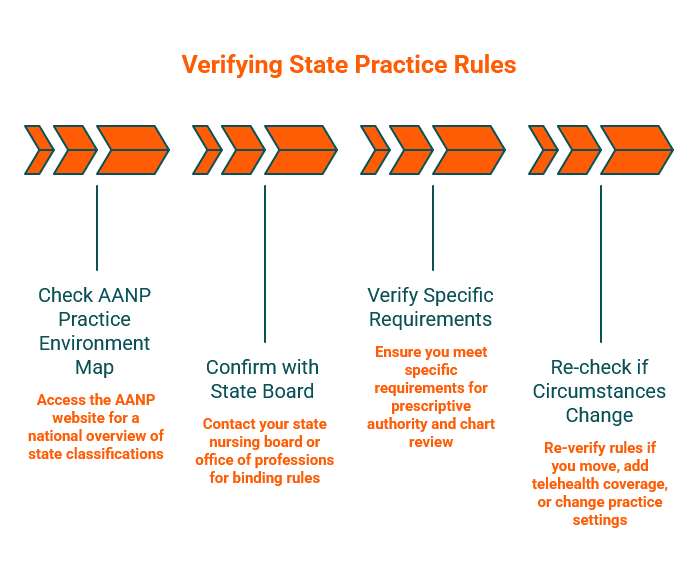
State rules change. Before launching, relocating, or adding telehealth patients in a new state, verify the current requirements using this four-step process:
Check the current AANP practice environment map. The AANP State Practice Environment page provides an up-to-date national overview of full, reduced, and restricted classifications. The 2026 map PDF offers a downloadable reference.
Confirm with your state board or office of professions. The AANP map is a starting point. Your state nursing board or office of professions publishes the binding rules. New York's Office of the Professions and New Jersey's APN certification page show why that second step matters.
Verify specific requirements tied to prescriptive authority, chart review, or written agreements. State classification tells you the category. Specific board rules tell you the paperwork.
Re-check if circumstances change. Moving states, adding telehealth coverage areas, or changing practice settings can all trigger new requirements.
When a Collaborating Physician Becomes a Practical Next Step
Collaboration is not always legally required—but it often becomes the clearest path to compliant, confident practice. Consider securing a collaborating physician if your state requires current collaboration for any element of your practice, if you are in a transition or threshold-based period and have not yet reached the experience requirement, if you are moving into a state with stricter requirements, or if you want a state-licensed physician match to ensure compliance certainty without the guesswork.
The key is finding a collaborator who holds a valid license in your specific state and understands your practice type. Once the category question is settled, Understanding the Collaborative Practice Agreement and Medical Director vs Collaborating Physician: What Each Role Actually Covers for Independent NPs help clarify what that structure should actually look like.
See the states Physician Collaborators currently covers to explore whether a match is available in your area.
FAQ
Is reduced practice the same as restricted practice?
No. Reduced practice means less than full authority, but the exact burden varies by state—it may involve a career-long collaborative agreement or limits tied to a setting or element of practice. Restricted practice requires career-long supervision, delegation, or team management for at least one element of care.
Can a reduced-practice state still require ongoing collaboration?
Yes. Some reduced-practice states, like New Jersey and Pennsylvania, require ongoing collaborative agreements that do not phase out with experience.
Does New York still require collaboration for newer NPs?
Yes. NPs with fewer than 3,600 hours of qualifying experience must have written practice protocols and a written practice agreement with a collaborating physician.
If I move states, do my collaboration requirements change?
They may. State category is location-specific, so a move or multi-state expansion can change the compliance model. Always verify the current requirements in your new state before practicing.
Where should I verify the current rule?
Start with the AANP State Practice Environment map, then confirm with your state board of nursing or office of professions.
Disclaimer: This article is for educational purposes only and is not legal, licensing, or financial advice. Nurse practitioner practice rules change over time and vary by state, setting, and prescriptive authority. Always verify the current requirements with your state board and qualified professional advisors before making operational decisions.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the Physician Collaborators Insights Team:
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.