
Physician Collaboration Agreement Clauses Independent NP Practices Should Review Before Signing
📌 Key Takeaways
A physician collaboration agreement should explain how the working relationship will run, not just name both parties.
Match State Rules: State law, license type, services, and patient location should shape the whole agreement.
Define Daily Roles: The agreement should spell out what the physician does beyond signing the document.
Document Real Contact: Calls, messages, chart reviews, and feedback need clear records for later review.
Plan For Change: New services, locations, telehealth states, or prescribing work may need a formal update.
Resolve Gaps Early: Vague terms about availability, chart review, escalation, or termination can create problems later.
Clear agreements protect the workflow before confusion reaches the clinic.
Independent NP practice owners will see what to check before signing, preparing them for the detailed overview that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
A physician collaboration agreement can look complete long before it is operationally useful. Independent NP practice owners often receive a proposed agreement with a start date approaching and a collaborating physician ready to move forward. The signature page is the easy part. The harder question is whether the agreement explains how collaboration will actually function in the practice: how the physician will be reachable, how chart review will be handled, how communication will be documented, and what happens when the practice changes.
Vague clauses do not create problems at signing. They surface when a real situation demands a clear answer the document cannot provide. The clauses below form a practical review framework — not legal advice, and not a substitute for qualified professional review. Because requirements vary meaningfully by state and practice type, verifying current obligations through official sources and counsel is essential.
Start With the Legal and Practice-Scope Requirements in Your State
Before reviewing individual clauses, establishing what the applicable state requires provides the necessary foundation. The American Association of Nurse Practitioners (updated 05/2026) describes three broad practice environment categories — full, reduced, and restricted — that determine the degree of physician involvement required. In reduced and restricted environments, a written agreement may be a condition of licensure or prescriptive authority. The NCSBN's APRN Consensus Model offers foundational context on how APRN regulation developed, though it should not be treated as current state-law guidance.
An agreement adequate for one practice may not address telehealth, controlled-substance prescribing, or a new service line. What the agreement must contain, whether it must be filed, and how chart review is defined require current verification through the relevant state board of nursing and applicable statutes. For practices operating across state lines, requirements may vary by patient location. The article on restricted vs. reduced practice states provides useful background on how location shapes these obligations.
One core question should anchor the entire review: does this agreement match the state, license, services, locations, and practice model the NP practice will actually use?
Use This Pre-Signature Clause Review Checklist
The table below organizes key clause areas into a structured review workflow. It is a preparation tool, not a legal sufficiency test. Use it to identify gaps and prepare specific questions before bringing the agreement to an attorney, compliance advisor, or collaboration provider.
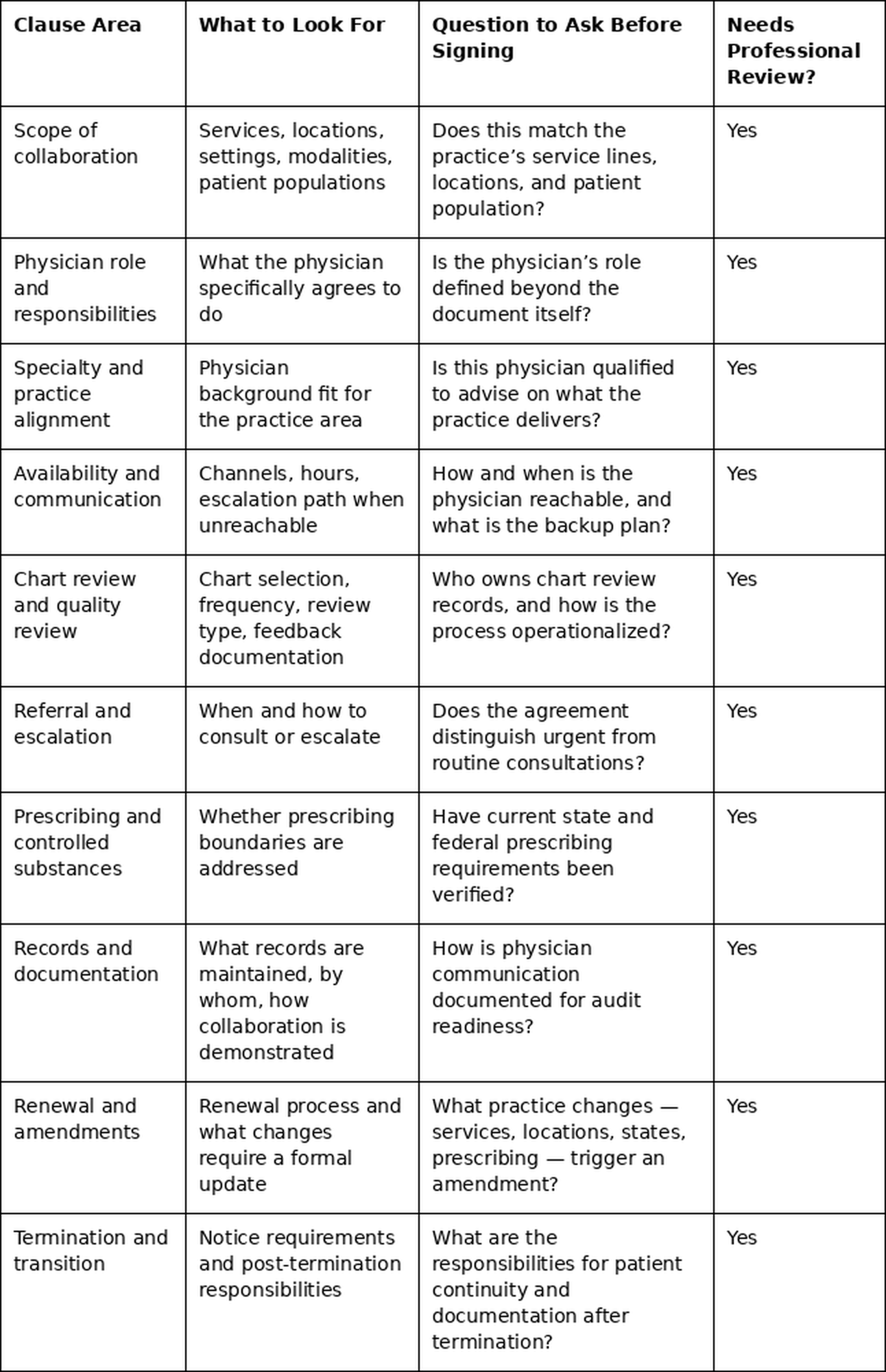
A useful agreement makes responsibilities easier to understand and document. If a clause raises more operational questions than it answers, that is a signal to flag it for review before signing — not after.
The Clauses That Deserve the Closest Review
Scope of Collaboration and Role Boundaries
The scope clause defines what the collaboration covers. It should identify which services, care settings, locations, and patient populations fall within the arrangement — and how the NP and physician are expected to interact around clinical questions.
This is also where practice-type fit becomes important. A broad clause may seem flexible, but it becomes difficult to use when neither party can identify what the physician is expected to review, discuss, or document. Physician Collaborators provides collaboration support for several practice types, including general medicine, behavioral health, telemedicine, urgent care, infusion therapy, integrative medicine, and med spa practices. Regardless of practice type, the legal and clinical details of any agreement still require professional review.
A hypothetical primary care NP opening a small independent practice might find that a borrowed template names the physician and lists broad service categories without describing how the two parties will communicate. The clause should be specific enough that both parties — and anyone reviewing documentation afterward — can understand how collaboration functions day to day.
Physician Availability and Communication Expectations
Availability should be more specific than "as needed." The agreement should specify communication channels — phone, secure messaging, email, or video — available hours, and the escalation path when the physician is unreachable.
What often receives less attention is documentation of meaningful communication. Demonstrating that collaboration is substantive, not nominal, requires a consistent record of consultations and physician responses — not just a list of available contact methods. Communication involving patient information should be handled consistently with applicable privacy and security obligations; HHS OCR's HIPAA Security Rule guidance is the authoritative starting point for that assessment, though practice-specific obligations should be confirmed with qualified compliance support.
Chart Review and Quality Review
The agreement should describe not only how often charts are reviewed but also the type: retrospective review of completed encounters, prospective review of planned care, random sampling, or focused review of a specific condition or risk area. Each serves a different quality assurance purpose.
For example, a practice that selects charts systematically, documents written physician feedback, and maintains dated records creates a far stronger accountability pattern than one where reviews occur informally without documentation. Physician Collaborators' FAQ notes that collaboration may include monthly sample chart review. Whether a specific frequency, sample size, or review type is required depends on state law and agreement terms, and should be confirmed through official sources and counsel.
Avoid assuming a universal percentage, frequency, or sampling method applies. Those details may vary by state, agreement, payer, policy, or practice model and should be verified before being treated as required.
Referral, Escalation, and Clinical Consultation
Escalation language defines when to consult the physician, how urgent questions differ from routine ones, and how consultations are documented. The agreement should clarify when the NP is expected to consult, refer, or escalate — not as a clinical treatment guide, but as an operational pathway for getting physician input when appropriate.
When working with a complex patient population, consistent documentation of each escalation — what prompted it, how the physician was reached, what guidance was given — creates an accountability record relevant to quality review and audit readiness. This clause does not replace clinical judgment; it makes that judgment traceable. If no one knows who documents the consultation, the process may be difficult to reconstruct later.
Prescribing and Controlled Substances
When the practice prescribes medications, particularly controlled substances, the agreement may need to address prescribing boundaries explicitly. Federal and state requirements apply simultaneously and can differ significantly. The DEA's Practitioner's Manual provides federal context but directs practitioners to current CSA regulations and Federal Register notices for complete requirements.
Adding controlled-substance prescribing illustrates a common gap: an agreement adequate before that expansion may be insufficient afterward, because collaboration obligations can change with prescribing authority. State law, licensing rules, registration requirements, and current federal updates may all be relevant and should be verified before treating any single source as definitive.
Records, Privacy, and Documentation Readiness
The agreement should help the practice understand what records need to be maintained. This may include chart review logs, communication records, meeting notes, written feedback, amendments, renewal records, and termination notices.
A useful framing question: if someone later asked how collaboration occurred, what records would show the process? Informal communication may be efficient in the moment, but without documentation it creates operational uncertainty that becomes difficult to resolve later. The agreement, related policies, or internal procedures should make clear where documentation belongs and who is responsible for maintaining it.
Renewal, Amendments, and Termination
The agreement should include a defined renewal process, a clear termination notice period, and an amendment mechanism for when practice circumstances change. Common triggers include adding a service line, opening a new care location, expanding telehealth to a new state, beginning controlled-substance prescribing, or transitioning to a new collaborating physician.
A hypothetical telehealth NP who begins seeing patients in a state not covered by the original agreement may be operating outside its stated scope — a risk the telehealth-ready collaborator article addresses in depth. Do not assume that an agreement signed for one version of the practice automatically fits the next version. Termination terms should also address how active patients are managed during any transition and how documentation responsibilities are allocated afterward.
Red Flags to Resolve Before Signing
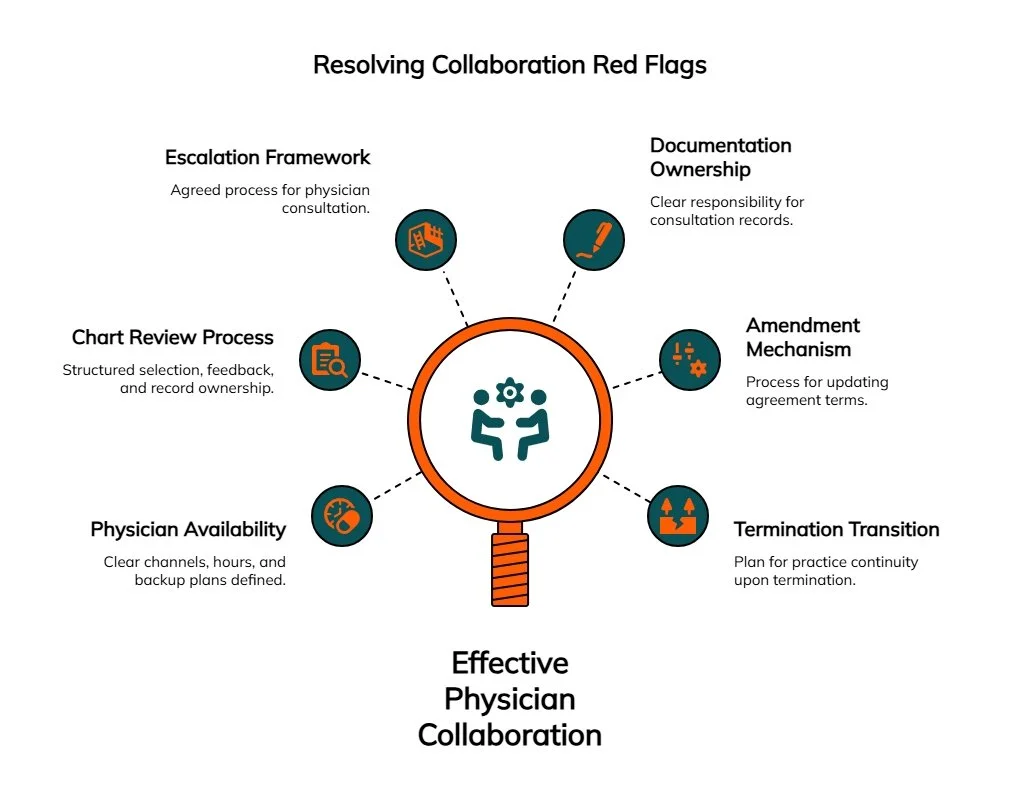
Some agreement problems are not about what is included but about what is absent or imprecise. The following patterns are worth resolving before signing:
Physician availability is undefined — channels, hours, and backup plans are unspecified.
Chart review exists in name only — no defined process for selection, feedback, or record ownership.
Escalation language is missing — no agreed framework for when and how to consult the physician.
Documentation ownership is unclear — uncertain who maintains records of consultations and communications.
No amendment mechanism — no process for updating when services, locations, states, or prescribing activity changes.
No termination transition plan — the arrangement can end without clear responsibility for practice continuity.
Agreement does not match the practice — a template from another state or specialty may not reflect actual needs.
Informal arrangements are not in writing — any understanding outside the document is a risk. The risks of informal supervisory agreements covers the legal and financial consequences in detail.
Speed replaced scrutiny — urgency around opening or renewing should not displace review of clauses that govern daily operations for months or years.
Role confusion is unresolved — a medical director and a collaborating physician carry different responsibilities depending on the practice and jurisdiction. If the agreement uses those terms loosely or interchangeably, review the distinction between a medical director and a collaborating physician before signing.
Questions to Bring to Your Attorney, Compliance Advisor, or Collaboration Provider
Arriving at professional review with specific questions makes the conversation more productive. A practical starting list:
Does this agreement meet the current requirements of the applicable state board of nursing and any relevant state medical board rules?
What does the physician specifically agree to do, and does that match the practice's clinical and operational needs?
How will chart review be documented — who selects charts, what type of review applies, and who maintains records?
What records should the practice maintain to demonstrate that active, meaningful collaboration is occurring?
How will urgent and non-urgent consultations be handled, and which channels are appropriate for patient-related communication?
What prescribing activities are included, limited, or excluded?
What practice changes require a formal amendment to this agreement?
What are the notice and transition responsibilities if either party ends the arrangement?
For collaboration process questions, Physician Collaborators' FAQ page provides a useful overview. If collaboration support is needed, request a free quote to discuss the practice's specific needs.
Frequently Asked Questions
What clauses should an NP review first in a physician collaboration agreement?
Start with scope, physician responsibilities, availability, chart review, documentation, referral and escalation, prescribing boundaries, renewal, amendment, and termination. These clauses affect how the agreement works in daily operations. The Pre-Signature Clause Review Checklist above provides a structured starting point for each area.
Is a physician collaboration agreement required in every state?
There is no single national answer. Requirements vary by state, practice authority, license, service model, and prescribing activities. Verify current requirements through official state sources and a qualified attorney or compliance advisor.
Should an attorney review a collaboration agreement before signing?
Attorney or qualified compliance review is strongly advisable for an independent NP practice. Agreement terms may affect state requirements, physician responsibilities, prescribing boundaries, documentation, and transition planning. A review framework prepares questions but does not substitute for professional analysis. The distinction between a medical director and a collaborating physician is a related question worth clarifying before the review.
Can a collaboration agreement guarantee compliance?
No. A well-structured agreement can support a compliance framework but does not replace current legal review, consistent documentation, and professional oversight. Requirements evolve, and an agreement adequate at signing may need updating as the practice or regulatory landscape changes.
How often should an NP practice review or update its collaboration agreement?
Review the agreement at renewal and whenever the practice changes in a meaningful way — adding a service line, opening a new location, expanding telehealth to a new state, beginning controlled-substance prescribing, or changing collaborating physicians. Required timing should be verified for the applicable state and practice model.
Is chart review always required?
Not universally. Whether chart review is required — and what form or frequency it must take — depends on state law, the specific agreement, payer requirements, and the collaboration model. Current requirements for the relevant jurisdiction should be confirmed through official state board guidance and professional consultation.
Review the Agreement Like a Workflow, Not a Form
The strongest physician collaboration agreement is not just signed — it is clear enough to use. The clauses that define scope, availability, chart review, escalation, prescribing boundaries, and termination describe how a collaboration will function across months and years of practice. Reviewing them before signing, with attention to what each clause means for real workflows and documentation, gives a clearer operational picture than a quick pass over the signature page.
That review belongs with qualified counsel and a compliance advisor. Practices evaluating collaboration support for their practice type or checking states where Physician Collaborators accepts applications will find additional resources available, including further reading on essential collaborative practice agreement clauses. A free consultation can help clarify what to look for before the agreement is finalized.
Disclaimer: This content is for informational purposes only. Laws, definitions, and deadlines change. Verify current requirements through official sources. This content is not legal, medical, or compliance advice. No attorney-client relationship is formed through this content. Please consult a qualified attorney in your jurisdiction for legal advice specific to your situation.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the Physician Collaborators Insights Team:
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice. This guide is intended as a comprehensive starting professional.