
Medical Director vs. Collaborating Physician: What Independent NPs Actually Need
📌 Key Takeaways
Most independent nurse practitioners need a collaborating physician for state compliance, not a medical director for organizational leadership.
Match the Role to Your Need: A collaborating physician handles chart review and clinical backup; a medical director runs policies and staff—paying for the wrong one wastes money.
Collaboration Costs Less: Collaborating physician fees typically run $500–$1,250 per month, while medical directors command higher rates for broader responsibilities.
State Rules Vary Widely: Some states require collaborative agreements, others grant full practice authority—verify your specific state's requirements before signing anything.
Specialty Fit Matters: A collaborating physician should practice in your clinical area; a mismatch creates compliance gaps during audits or board reviews.
Read the Agreement Carefully: Check chart review frequency, availability hours, communication methods, and termination terms before committing.
Don't pay for a title—pay for the compliance your practice actually needs.
Independent nurse practitioners and physician assistants launching or running their own practices will find clear guidance here, preparing them for the detailed comparison that follows.
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
The title on the contract matters less than what it actually covers. For many independent nurse practitioners, the real question isn't which role sounds more authoritative—it's which arrangement satisfies state compliance requirements without draining practice revenue on unnecessary overhead.
Most independent NP practices need compliant physician collaboration, not a medical director title. The distinction protects both your license and your bottom line. Requirements vary by state and practice model, so verifying what applies to your specific situation is essential before signing any agreement.
The Short Answer: Which Role Do Most Independent NPs Need?
A collaborating physician typically fulfills the oversight requirements that state boards mandate for independent NP practice. This contracted partnership provides the chart review, clinical availability, and compliance documentation that keeps your practice legally operational.
A medical director, by contrast, usually implies a broader organizational leadership function. That role often comes with employment-style arrangements, policy-setting responsibilities, and significantly higher costs.
For a solo telehealth practice or small independent clinic, paying for executive-level medical leadership when you actually need state-mandated collaboration creates what some practitioners call a "title tax"—overhead that doesn't match the operational need.
State practice environments differ substantially. The AANP State Practice Environment resource provides a starting point for understanding where your state falls on the spectrum of full practice authority versus reduced or restricted practice requirements.
Medical Director vs. Collaborating Physician: Side-by-Side Comparison
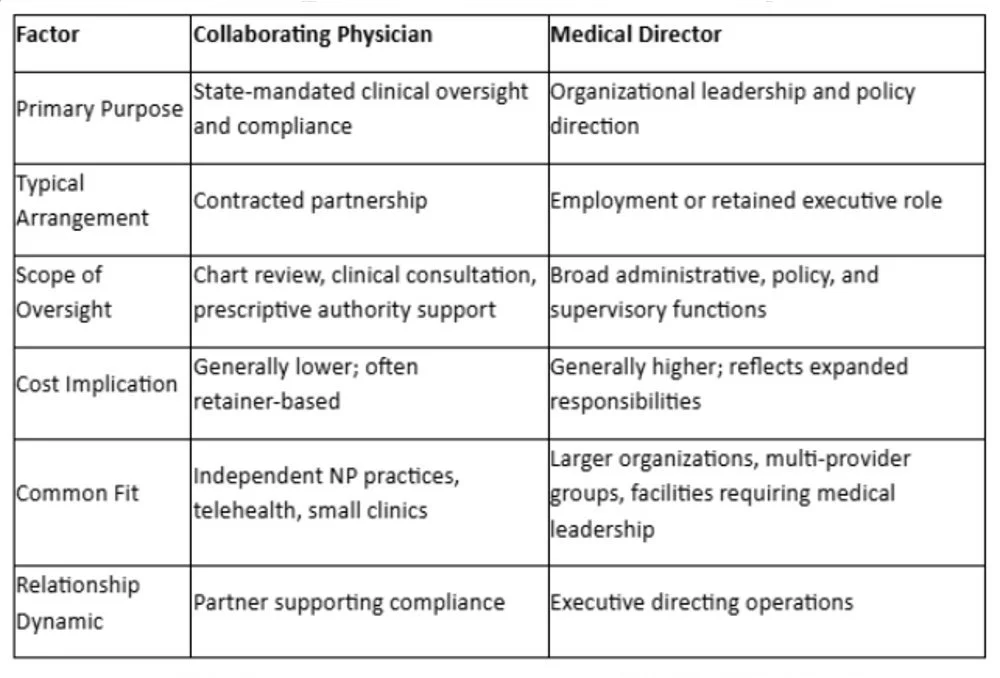
The chart above captures general distinctions. Actual arrangements vary based on state regulations, practice type, and individual agreements. Before committing, verify current requirements with your state board and review any agreement with qualified legal counsel.
What a Collaborating Physician Usually Covers
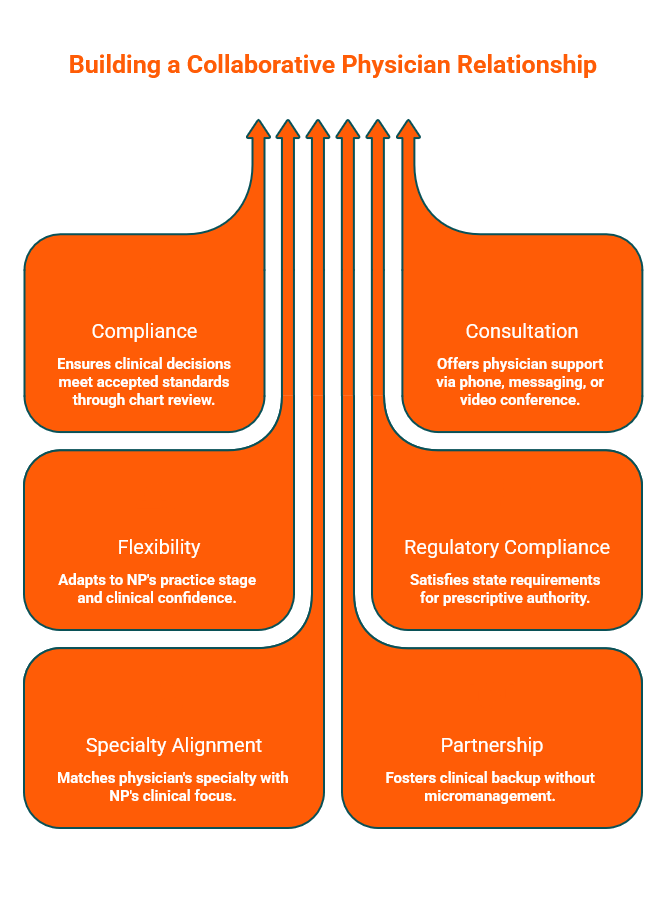
A collaborating physician serves as a compliance partner rather than an employer or supervisor. The arrangement typically includes periodic chart review—often a sample of patient records each month—to ensure clinical decision-making aligns with accepted standards.
Availability for consultation is another core component. When clinical questions arise, having access to a board-certified physician via phone, encrypted messaging, or video conference provides both practical support and documentation of oversight. This access typically occurs during regular business hours, though specific terms depend on the agreement.
The level of involvement can flex to match your needs. Some practitioners benefit from hands-on guidance, while others need only lighter administrative oversight. A good collaboration arrangement adjusts to your practice stage and clinical confidence rather than imposing a rigid structure.
For NPs in states requiring collaborative practice agreements for prescriptive authority, the collaborating physician provides the licensed physician relationship that satisfies regulatory requirements. Understanding the essential clauses in a collaborative practice agreement helps ensure your arrangement covers what your state actually mandates.
Specialty alignment matters here. A collaborating physician practicing in Internal Medicine, Family Medicine, Emergency Medicine, or Psychiatry should match the clinical focus of your practice. This extends across diverse practice models, from general medicine and behavioral health to specialized telehealth platforms. A mismatch creates compliance gaps that can surface during audits or board inquiries.
The relationship works when it feels like a partnership—clinical backup without micromanagement.
Costs for collaborating physician arrangements typically range from $500–$1,250 per month depending on your specific practice, according to Physician Collaborators' stated pricing. That range should be treated as one company's benchmark rather than a market-wide standard.
When a Medical Director Might Actually Make Sense
Not every practice fits the collaborating physician model. Some organizational structures genuinely require medical director involvement.
Larger multi-provider practices often need someone responsible for clinical protocols, quality assurance programs, and staff oversight that extends beyond individual chart review. Facilities like urgent care centers, infusion therapy clinics, or med spas may have regulatory or operational requirements calling for formal medical direction.
If your practice model involves supervising other clinicians, developing institutional policies, or representing the organization in medical staff functions, a medical director role addresses those responsibilities. The cost reflects the expanded scope.
The mistake isn't hiring a medical director when you need one. The mistake is assuming the more senior-sounding title automatically provides better protection. It doesn't. It provides different coverage for different needs.
Clarifying whether you need compliance support or organizational leadership prevents overspending on a role that doesn't fit your practice structure.
A 5-Question Decision Check Before You Sign
Before entering any physician oversight arrangement, work through these questions:
1. What does my state actually require?
State boards define whether collaborative agreements, supervisory relationships, or full practice authority applies to your license. Requirements for prescriptive authority often have additional stipulations. Verify current regulations directly with your state board.
The AANP State Practice Environment map shows how state laws affect NP practice and serves as a useful starting point. For state-specific verification, consult official sources such as the New York State Education Department NP practice requirements, New Jersey APN certification guidance, or Pennsylvania's collaborative agreement guide.
2. Is my need clinical collaboration or broader operational leadership?
If the answer is chart review, consultation access, and compliance documentation, a collaborating physician likely fits. If you need someone setting protocols and directing clinical staff, the scope expands.
3. Am I paying for compliance or for hierarchy?
A contracted collaborator satisfies regulatory mandates. An employed medical director builds organizational infrastructure. Both have value in the right context. Paying for infrastructure you don't need drains resources that could support practice growth.
4. Does this arrangement fit my specialty and practice model?
A collaborator practicing Family Medicine may not align with a behavioral health-focused telehealth practice. Specialty fit affects both compliance defensibility and the quality of clinical support you receive.
5. What exactly is inside the agreement?
Review the specifics: chart review frequency, availability windows, communication methods, termination terms, and malpractice considerations. A faster match isn't always a better match if the agreement doesn't fit your practice.
Common Mistakes That Create a Title Tax
Paying for prestige instead of need tops the list. The more senior-sounding title creates a false sense of security if it doesn't actually address your compliance requirements.
Assuming one title is universally required leads to expensive mismatches. A practice in a full practice authority state has different needs than one in a restricted practice state. Treating collaboration requirements as uniform across all jurisdictions invites both overspending and compliance gaps.
Skipping state-specific verification creates downstream problems. Regulations change. What applied when a colleague launched their practice may not reflect current requirements. Confirm with official sources before structuring your arrangement.
Ignoring specialty or practice-fit issues undermines the collaboration itself. A collaborating physician who doesn't understand your patient population or clinical focus provides limited practical support.
Confusing thin oversight with savings may look inexpensive upfront but can become costly. A low-cost arrangement that doesn't provide usable support, genuine fit, or clear agreement terms may create liability exposure rather than real savings.
The right collaborating physician accelerates practice growth because the relationship provides genuine clinical partnership—not just a signature.
Don't pay for a title. Pay for the compliance you actually need.
Ready to find the right fit? Get a free quote for a collaborating physician matched to your specialty and state. The consultation covers your degree, state, malpractice coverage, practice type, controlled-substances status, and NPI. Physician Collaborators responds within 24 hours, with matching typically completed within one week.
Disclaimer: This article is for informational purposes only and does not constitute legal, regulatory, or medical-practice advice. Because nurse practitioner collaboration and oversight requirements vary by state, specialty, and practice model, readers should verify current requirements with the relevant state board and qualified legal or compliance professionals.
Our Editorial Process:
Our expert team uses AI tools to help organize and structure our initial drafts. Every piece is then extensively rewritten, fact-checked, and enriched with first-hand insights and experiences by expert humans on our Insights Team to ensure accuracy and clarity.
About the Physician Collaborators Insights Team:
The Physician Collaborators Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice. This guide is intended as a comprehensive starting point. For decisions specific to your unique situation, we always recommend consulting a qualified professional.